

Coronavirus Disease 2019-Associated PICU Admissions: A Report From the Society of Critical Care Medicine Discovery Network Viral Infection and Respiratory Illness Universal Study Registry
- PMID: 33965987
- PMCID: PMC8240492
- DOI: 10.1097/PCC.0000000000002760
Coronavirus Disease 2019-Associated PICU Admissions: A Report From the Society of Critical Care Medicine Discovery Network Viral Infection and Respiratory Illness Universal Study Registry
Abstract
Objectives: To compare clinical characteristics and outcomes of children admitted to the PICU for severe acute respiratory syndrome coronavirus 2-related illness with or without multisystem inflammatory syndrome in children. The secondary objective was to identify explanatory factors associated with outcome of critical illness defined by a composite index of in-hospital mortality and organ system support requirement.
Design: Retrospective cohort study.
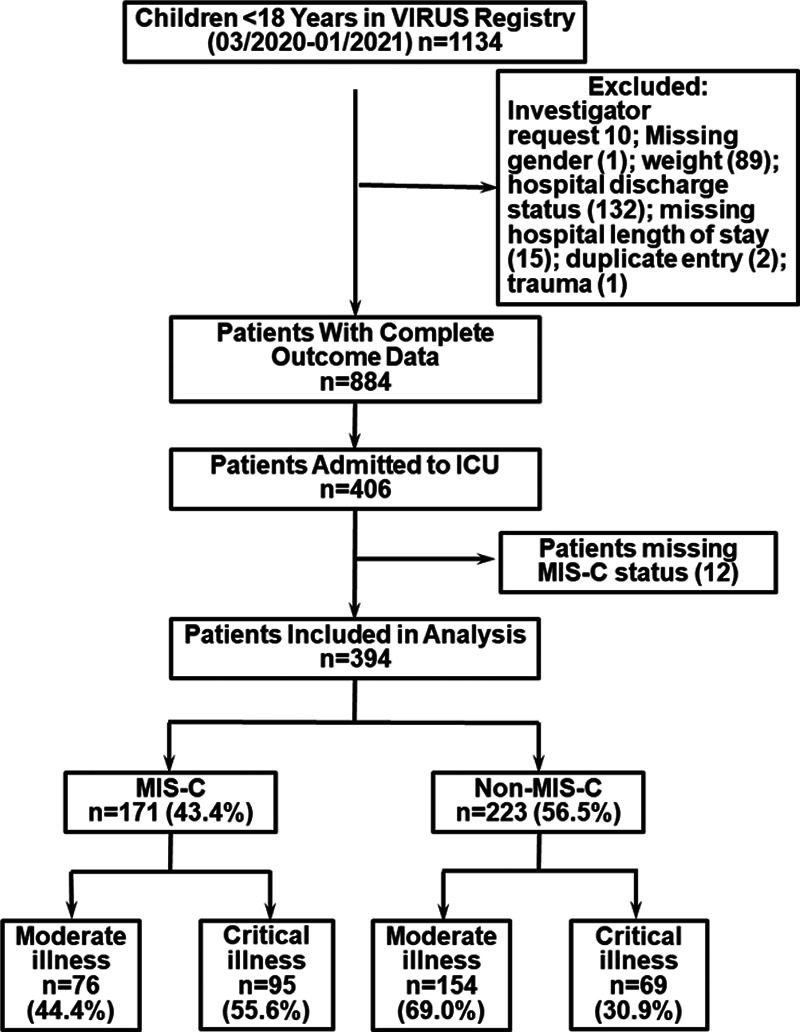
Setting: Thirty-eight PICUs within the Viral Infection and Respiratory Illness Universal Study registry from March 2020 to January 2021.
Patients: Children less than 18 years with severe acute respiratory syndrome coronavirus 2-related illness with or without multisystem inflammatory syndrome in children.
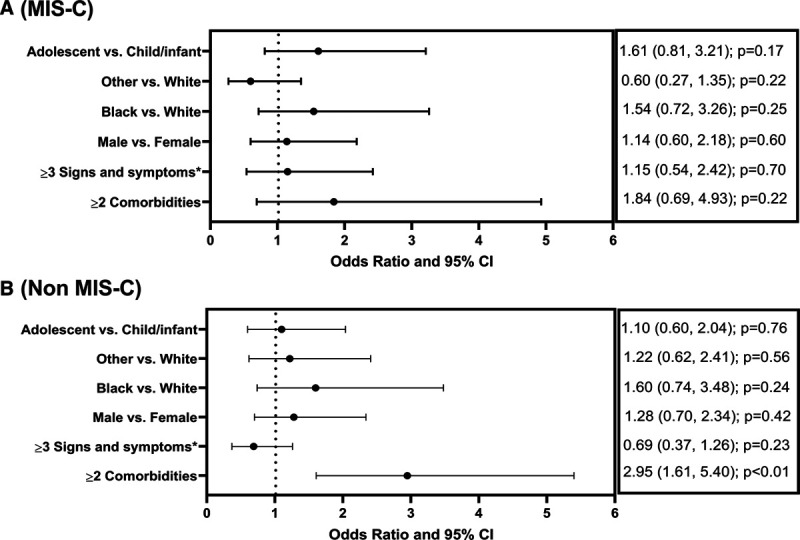
Measurements and main results: Of 394 patients, 171 (43.4%) had multisystem inflammatory syndrome in children. Children with multisystem inflammatory syndrome in children were more likely younger (2-12 yr vs adolescents; p < 0.01), Black (35.6% vs 21.9%; p < 0.01), present with fever/abdominal pain than cough/dyspnea (p < 0.01), and less likely to have comorbidities (33.3% vs 61.9%; p < 0.01) compared with those without multisystem inflammatory syndrome in children. Inflammatory marker levels, use of inotropes/vasopressors, corticosteroids, and anticoagulants were higher in multisystem inflammatory syndrome in children patients (p < 0.01). Overall mortality was 3.8% (15/394), with no difference in the two groups. Diagnosis of multisystem inflammatory syndrome in children was associated with longer duration of hospitalization as compared to nonmultisystem inflammatory syndrome in children (7.5 d[interquartile range, 5-11] vs 5.3 d [interquartile range, 3-11 d]; p < 0.01). Critical illness occurred in 164 patients (41.6%) and was more common in patients with multisystem inflammatory syndrome in children compared with those without (55.6% vs 30.9%; p < 0.01). Multivariable analysis failed to show an association between critical illness and age, race, sex, greater than or equal to three signs and symptoms, or greater than or equal to two comorbidities among the multisystem inflammatory syndrome in children cohort. Among nonmultisystem inflammatory syndrome in children patients, the presence of greater than or equal to two comorbidities was associated with greater odds of critical illness (odds ratio 2.95 [95% CI, 1.61-5.40]; p < 0.01).
Conclusions: This study delineates significant clinically relevant differences in presentation, explanatory factors, and outcomes among children admitted to PICU with severe acute respiratory syndrome coronavirus 2-related illness stratified by multisystem inflammatory syndrome in children.
Copyright © 2021 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.
Conflict of interest statement
Dr. Bjornstad’s institution received funding from the International Society of Nephrology and Bioporto. Drs. Kashyap’s, Ms. Boman’s, Dr. Kumar’s institutions received funding from The Gordon and Betty Moore Foundation. Drs. Kashyap’s, Ms. Boman’s, and Dr. Kumar’s institutions received funding from Janssen and Janssen LLC. Dr. Kashyap receives funding from the National Institutes of Health (NIH)/National Heart, Lung and Blood Institute: R01HL 130881, UG3/UH3HL 141722; Gordon and Betty Moore Foundation Janssen Research and Development, LLC; and royalties from Ambient Clinical Analytics. Inc. Dr. Chiotos funded by Agency for Healthcare Research and Quality (K12-HS026393). Dr. Heneghan’s institution received funding from Society of Critical Care Medicine (SCCM). Dr Zimmerman’s institution received funding from the NIH, Immunexpress, Seattle, and he received funding from Elsevier Publishing Company. Dr. Kumar receives funding from the Gordon and Betty Moore Foundation, Centers for Disease Control and Prevention Foundation through the University of Washington, and Janssen Research and Development, LLC. Dr. Bhalala currently funded by NIH (site-principal investigator [PI] for Stress Hydrocortisone in Pediatric Septic Shock—R01HD096901), The Children’s Hospital of Philadelphia (site-PI for Pediatric Resuscitation Quality Collaborative), Voelcker Pilot Grant (PI for a project on prearrest electrocardiographic changes), The Children’s Hospital of San Antonio Endowed Chair Funds for ancillary projects related to SCCM Viral Infection and Respiratory Illness Universal Study (VIRUS) (coronavirus disease 2019) Registry and SCCM VIRUS electronic medical record automation pilot. The remaining authors have disclosed that they do not have any potential conflicts of interest.
Figures
References
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
