

A UK nationwide study of people with type 1 diabetes admitted to hospital with COVID-19 infection
- PMID: 33966090
- PMCID: PMC8106514
- DOI: 10.1007/s00125-021-05463-x
A UK nationwide study of people with type 1 diabetes admitted to hospital with COVID-19 infection
Abstract
Aims/hypothesis: The aim of this work was to describe the clinical characteristics of adults with type 1 diabetes admitted to hospital and the risk factors associated with severe coronavirus disease-2019 (COVID-19) in the UK.
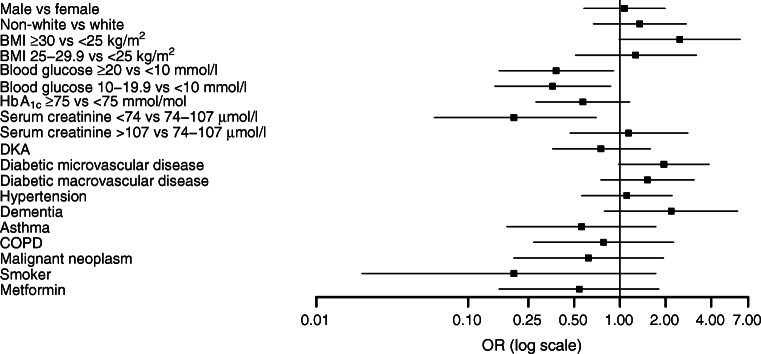
Methods: A retrospective cohort study was performed using data collected through a nationwide audit of people admitted to hospital with diabetes and COVID-19, conducted by the Association of British Clinical Diabetologists from March to October 2020. Prespecified demographic, clinical, medication and laboratory data were collected from the electronic and paper medical record systems of the participating hospitals by local clinicians. The primary outcome of the study, severe COVID-19, was defined as death in hospital and/or admission to the adult intensive care unit (AICU). Logistic regression models were used to generate age-adjusted ORs.
Results: Forty UK centres submitted data. The final dataset included 196 adults who were admitted to hospital and had both type 1 diabetes and COVID-19 on admission (male sex 55%, white 70%, with mean [SD] age 62 [19] years, BMI 28.3 [7.3] kg/m2 and last recorded HbA1c 76 [31] mmol/mol [9.1 (5.0)%]). The prevalence of pre-existing microvascular disease and macrovascular disease was 56% and 39%, respectively. The prevalence of diabetic ketoacidosis on admission was 29%. A total of 68 patients (35%) died or were admitted to AICU. The proportions of people that died were 7%, 38% and 38% of those aged <55, 55-74 and ≥75 years, respectively. BMI, serum creatinine levels and having one or more microvascular complications were positively associated with the primary outcome after adjusting for age.
Conclusions/interpretation: In people with type 1 diabetes and COVID-19 who were admitted to hospital in the UK, higher BMI, poorer renal function and presence of microvascular complications were associated with greater risk of death and/or admission to AICU. Risk of severe COVID-19 is reassuringly very low in people with type 1 diabetes who are under 55 years of age without microvascular or macrovascular disease. IN PEOPLE WITH TYPE 1 DIABETES AND COVID-19 ADMITTED TO HOSPITAL IN THE UK, BMI AND ONE OR MORE MICROVASCULAR COMPLICATIONS HAD A POSITIVE ASSOCIATION AND LOW SERUM CREATINE LEVELS HAD A NEGATIVE ASSOCIATION WITH DEATH/ADMISSION TO INTENSIVE CARE UNIT AFTER ADJUSTING FOR AGE.
Keywords: COVID-19; Inpatients; Mortality; National audit; Type 1 diabetes.
Figures
References
-
- Worldometer. Coronavirus. Available from: www.worldometers.info/coronavirus. Accesed 15 Dec 2020
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
