

Continuous subcutaneous insulin infusion therapy is associated with reduced retinopathy progression compared with multiple daily injections of insulin
- PMID: 33966091
- PMCID: PMC8245368
- DOI: 10.1007/s00125-021-05456-w
Continuous subcutaneous insulin infusion therapy is associated with reduced retinopathy progression compared with multiple daily injections of insulin
Abstract
Aims/hypothesis: We aimed to compare diabetic retinopathy outcomes in people with type 1 diabetes following introduction of continuous subcutaneous insulin infusion (CSII) therapy with outcomes in people receiving continuing therapy with multiple daily insulin injections (MDI).
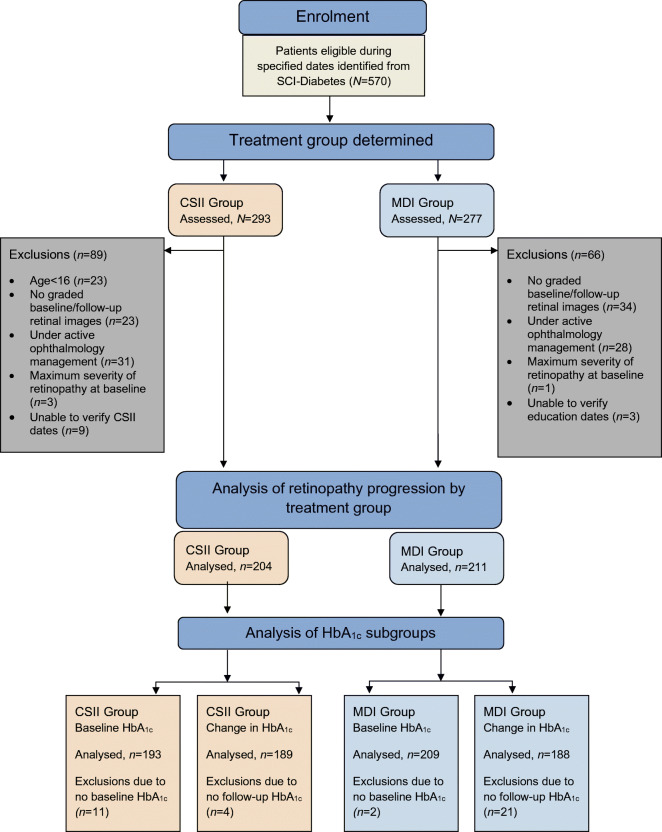
Methods: This is a retrospective cohort study using the Scottish Care Information - Diabetes database for retinal screening outcomes and HbA1c changes in 204 adults commenced on CSII therapy between 2013 and 2016, and 211 adults eligible for CSII during the same period but who continued on MDI therapy. Diabetic retinopathy progression (time to minimum one-grade worsening in diabetic retinopathy from baseline grading) was plotted for CSII and MDI cohorts using Kaplan-Meier curves, and outcomes were compared using multivariate Cox regression analysis adjusting for age, sex, baseline HbA1c, blood pressure, cholesterol, smoking status and socioeconomic quintile. Impact of baseline HbA1c and change in HbA1c on diabetic retinopathy progression was assessed within CSII and MDI cohorts.
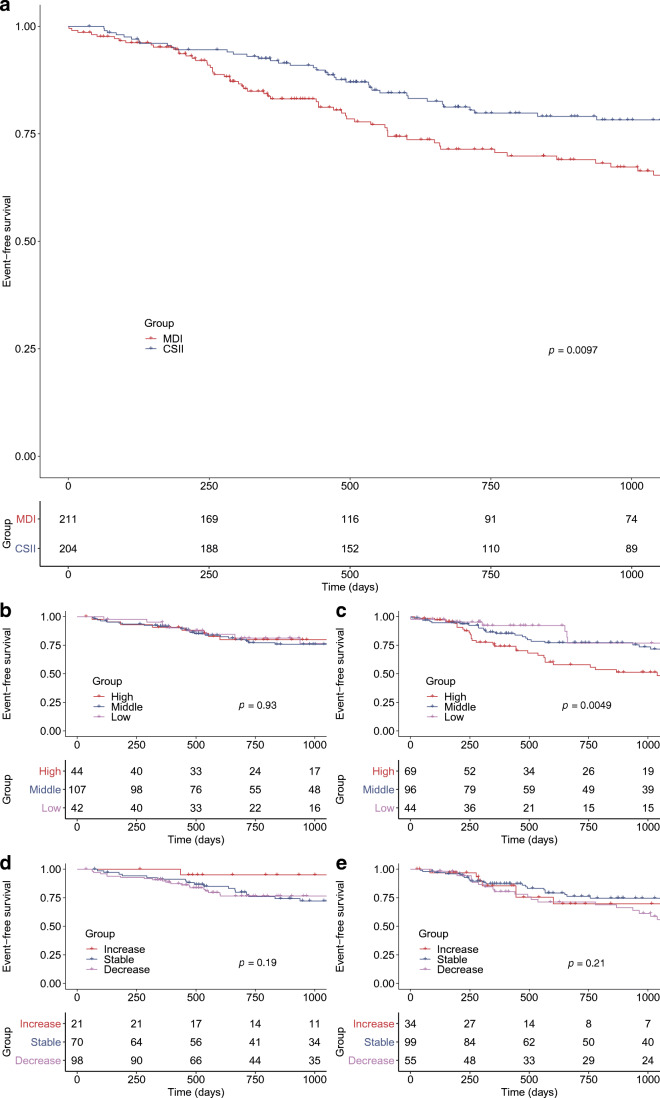
Results: CSII participants were significantly younger, were from less socially deprived areas, and had lower HbA1c and higher diastolic BP at baseline. There was a larger reduction in HbA1c at 1 year in those on CSII vs MDI (-6 mmol/mol [-0.6%] vs -2 mmol/mol [-0.2%], p < 0.01). Diabetic retinopathy progression occurred in a smaller proportion of adults following commencement of CSII vs continued MDI therapy over mean 2.3 year follow-up (26.5% vs 18.6%, p = 0.0097). High baseline HbA1c (75 mmol/mol [9%]) was associated with diabetic retinopathy progression in the MDI group (p = 0.0049) but not the CSII group (p = 0.93). Change in HbA1c at follow-up, irrespective of baseline glycaemic status, did not significantly affect diabetic retinopathy progression in either group.
Conclusions/interpretation: CSII was associated with reduced diabetic retinopathy progression compared with continued MDI therapy, and may be protective against diabetic retinopathy progression for those with high baseline HbA1c. Progression of diabetic retinopathy over 3 years was not associated with a change in HbA1c.
Keywords: Clinical diabetes; Clinical science; Insulin therapy; Microvascular complications; Retinopathy.
Figures
Similar articles
-
Continuous subcutaneous insulin infusion versus multiple daily injections in children and young people at diagnosis of type 1 diabetes: the SCIPI RCT.Health Technol Assess. 2018 Aug;22(42):1-112. doi: 10.3310/hta22420. Health Technol Assess. 2018. PMID: 30109847 Free PMC article. Clinical Trial.
-
Continuous subcutaneous insulin infusion versus multiple daily injection regimens in children and young people at diagnosis of type 1 diabetes: pragmatic randomised controlled trial and economic evaluation.BMJ. 2019 Apr 3;365:l1226. doi: 10.1136/bmj.l1226. BMJ. 2019. PMID: 30944112 Free PMC article. Clinical Trial.
-
Long-term body weight trajectories and metabolic control in type 1 diabetes patients on insulin pump or multiple daily injections: A 10-year retrospective controlled study.Nutr Metab Cardiovasc Dis. 2019 Oct;29(10):1110-1117. doi: 10.1016/j.numecd.2019.06.008. Epub 2019 Jun 20. Nutr Metab Cardiovasc Dis. 2019. PMID: 31371264
-
Glycemic Control During Continuous Subcutaneous Insulin Infusion Versus Multiple Daily Insulin Injections in Type 2 Diabetes: Individual Patient Data Meta-analysis and Meta-regression of Randomized Controlled Trials.Diabetes Care. 2017 May;40(5):715-722. doi: 10.2337/dc16-2201. Diabetes Care. 2017. PMID: 28428322 Review.
-
Optimizing type 1 diabetes after multiple daily injections and capillary blood monitoring: Pump or sensor first? A meta-analysis using pooled differences in outcome measures.Diabetes Obes Metab. 2021 Nov;23(11):2521-2528. doi: 10.1111/dom.14498. Epub 2021 Aug 12. Diabetes Obes Metab. 2021. PMID: 34286892
Cited by
-
Use of Diabetes Technologies and Retinopathy in Adults With Type 1 Diabetes.JAMA Netw Open. 2024 Mar 4;7(3):e240728. doi: 10.1001/jamanetworkopen.2024.0728. JAMA Netw Open. 2024. PMID: 38446483 Free PMC article.
-
The impact of insulin pump therapy compared to multiple daily injections on complications and mortality in type 1 diabetes: A real-world retrospective cohort study.Diabetes Obes Metab. 2025 Aug;27(8):4239-4247. doi: 10.1111/dom.16455. Epub 2025 May 19. Diabetes Obes Metab. 2025. PMID: 40390300 Free PMC article.
-
Delivering evidence-based interventions for type 1 diabetes in the virtual world - A review of UK practice during the SARS-CoV-2 pandemic.Diabetes Res Clin Pract. 2022 Mar;185:109777. doi: 10.1016/j.diabres.2022.109777. Epub 2022 Feb 11. Diabetes Res Clin Pract. 2022. PMID: 35157943 Free PMC article. Review.
-
RETINAL MICROVASCULOPATHY WITH DIFFERENT INSULIN INFUSION THERAPIES IN CHILDREN WITH TYPE 1 DIABETES MELLITUS WITHOUT CLINICAL DIABETIC RETINOPATHY.Retina. 2024 May 1;44(5):895-900. doi: 10.1097/IAE.0000000000004028. Epub 2024 Apr 18. Retina. 2024. PMID: 38127867 Free PMC article.
-
Continuous Glucose Monitor, Insulin Pump, and Automated Insulin Delivery Therapies for Type 1 Diabetes: An Update on Potential for Cardiovascular Benefits.Curr Cardiol Rep. 2022 Dec;24(12):2043-2056. doi: 10.1007/s11886-022-01799-x. Epub 2022 Oct 24. Curr Cardiol Rep. 2022. PMID: 36279036 Free PMC article. Review.
References
-
- Diabetic Retinopathy Guidelines Expert Working Party (2012) The Royal College of Ophthalmologists Diabetic Retinopathy Guidelines December 2012. Available from https://www.rcophth.ac.uk/wp-content/uploads/2014/12/2013-SCI-301-FINAL-.... Accessed 10 Jun 2020
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
