

Hemostatic Efficacy and Anti-FXa (Factor Xa) Reversal With Andexanet Alfa in Intracranial Hemorrhage: ANNEXA-4 Substudy
- PMID: 33966491
- PMCID: PMC8140631
- DOI: 10.1161/STROKEAHA.120.030565
Hemostatic Efficacy and Anti-FXa (Factor Xa) Reversal With Andexanet Alfa in Intracranial Hemorrhage: ANNEXA-4 Substudy
Erratum in
-
Correction to: Hemostatic Efficacy and Anti-FXa (Factor Xa) Reversal With Andexanet Alfa in Intracranial Hemorrhage: ANNEXA-4 Substudy.Stroke. 2021 Aug;52(8):e525. doi: 10.1161/STR.0000000000000386. Epub 2021 Jul 26. Stroke. 2021. PMID: 34310182 Free PMC article. No abstract available.
Abstract
Background and purpose: Andexanet alfa is a recombinant modified human FXa (factor Xa) developed to reverse FXa inhibition from anticoagulants. Hemostatic efficacy and reversal of anti-FXa activity with andexanet were assessed in patients from the ANNEXA-4 study (Andexanet Alfa, a Novel Antidote to the Anticoagulation Effects of FXa Inhibitors) with intracranial hemorrhage (ICrH).
Methods: ANNEXA-4 was a single-arm study evaluating andexanet in patients presenting with major bleeding ≤18 hours after taking an FXa inhibitor. Patients received a bolus plus 2-hour infusion of andexanet. Brain imaging in patients with ICrH was performed at baseline and at 1 and 12 hours postandexanet infusion. Coprimary efficacy outcomes were change in anti-FXa activity and hemostatic efficacy at 12 hours (excellent/good efficacy defined as ≤35% increase in hemorrhage volume/thickness). Safety outcomes included occurrence of thrombotic events and death at 30 days.
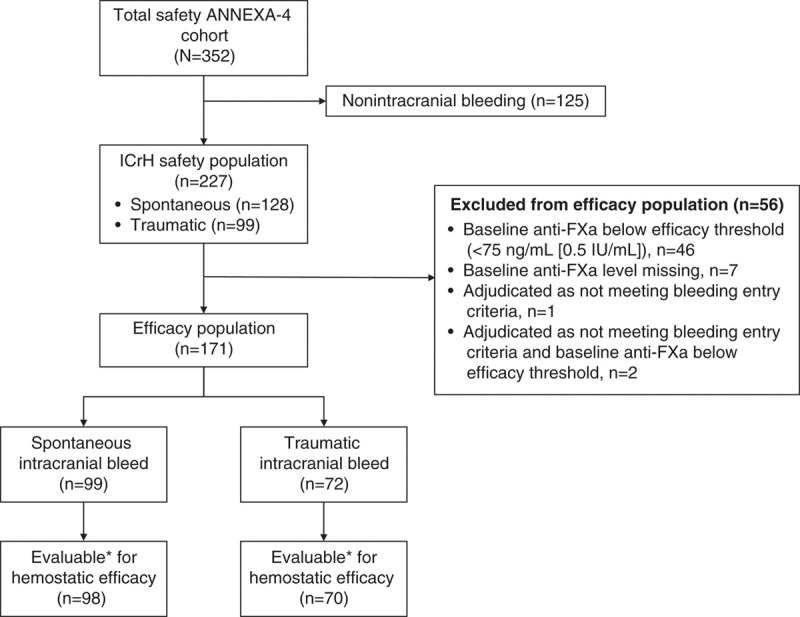
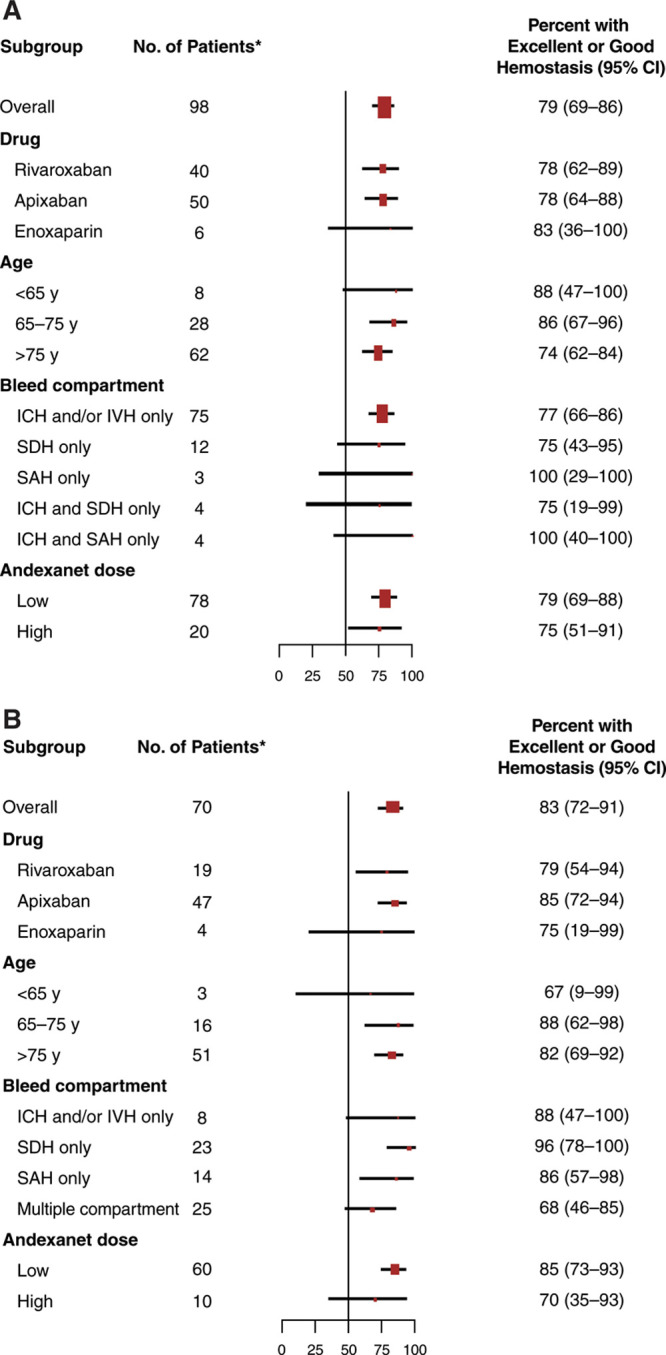
Results: A total of 227 patients with ICrH were included in the safety population (51.5% male; mean age 79.3 years) and 171 in the efficacy population (99 spontaneous and 72 traumatic bleeds). In efficacy evaluable patients, excellent/good hemostasis 12 hours postandexanet occurred in 77 out of 98 (78.6%) and in 58 out of 70 (82.9%) patients with spontaneous and traumatic bleeding, respectively. In the subanalysis by FXa inhibitor treatment group in the efficacy population, median of percent change in anti-FXa from baseline to nadir showed a decrease of 93.8% for apixaban-treated patients (n=99) and by 92.6% for rivaroxaban-treated patients (n=59). Within 30 days, death occurred in 34 out of 227 (15.0%) patients and thrombotic events occurred in 21 out of 227 (9.3%) patients (safety population).
Conclusions: Andexanet reduced anti-FXa activity in FXa inhibitor-treated patients with ICrH, with a high rate of hemostatic efficacy. Andexanet may substantially benefit patients with ICrH, the most serious complication of anticoagulation.
Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT02329327.
Keywords: andexanet alfa; direct factor Xa inhibitor reversal; intracranial hemorrhage.
Figures
Comment in
-
Evidence for Andexanet Alpha in Reversing Intracerebral Hemorrhage due to Factor Xa Inhibitors?Stroke. 2021 Jun;52(6):2106-2108. doi: 10.1161/STROKEAHA.120.031825. Epub 2021 May 10. Stroke. 2021. PMID: 33966496 No abstract available.
References
-
- Granger CB, Alexander JH, McMurray JJ, Lopes RD, Hylek EM, Hanna M, Al-Khalidi HR, Ansell J, Atar D, Avezum A, et al. ; ARISTOTLE Committees and Investigators. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365:981–992. doi: 10.1056/NEJMoa1107039 - PubMed
-
- Patel MR, Mahaffey KW, Garg J, Pan G, Singer DE, Hacke W, Breithardt G, Halperin JL, Hankey GJ, Piccini JP, et al. ; ROCKET AF Investigators. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365:883–891. doi: 10.1056/NEJMoa1009638 - PubMed
-
- Giugliano RP, Ruff CT, Braunwald E, Murphy SA, Wiviott SD, Halperin JL, Waldo AL, Ezekowitz MD, Weitz JI, Špinar J, et al. ; ENGAGE AF-TIMI 48 Investigators. Edoxaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2013;369:2093–2104. doi: 10.1056/NEJMoa1310907 - PubMed
-
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, Castella M, Diener HC, Heidbuchel H, Hendriks J, et al. ; ESC Scientific Document Group. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37:2893–2962. doi: 10.1093/eurheartj/ehw210 - PubMed
-
- January CT, Wann LS, Alpert JS, Calkins H, Cigarroa JE, Cleveland JC, Jr, Conti JB, Ellinor PT, Ezekowitz MD, Field ME, et al. ; ACC/AHA Task Force Members. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation. 2014;130:e199–e267. doi: 10.1161/CIR.0000000000000041 - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
