

Multimodal assessment of right ventricle overload-metabolic and clinical consequences in pulmonary arterial hypertension
- PMID: 33966635
- PMCID: PMC8108462
- DOI: 10.1186/s12968-021-00743-2
Multimodal assessment of right ventricle overload-metabolic and clinical consequences in pulmonary arterial hypertension
Abstract
Background: In pulmonary arterial hypertension (PAH) increased afterload leads to adaptive processes of the right ventricle (RV) that help to maintain arterio-ventricular coupling of RV and preserve cardiac output, but with time the adaptive mechanisms fail. In this study, we propose a multimodal approach which allows to estimate prognostic value of RV coupling parameters in PAH patients.
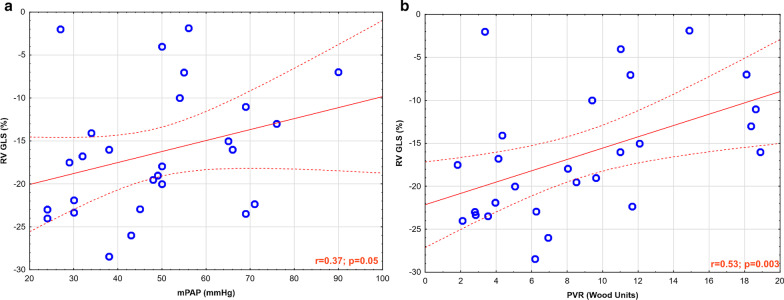
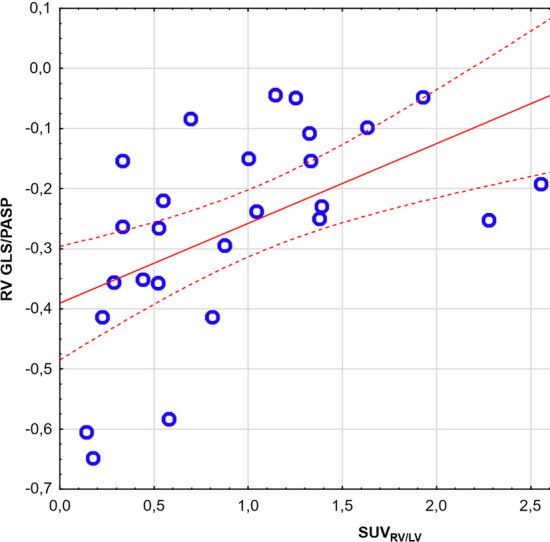
Methods: Twenty-seven stable PAH patients (49.5 ± 15.5 years) and 12 controls underwent cardiovascular magnetic resonance (CMR). CMR feature tracking analysis was performed for RV global longitudinal strain assessment (RV GLS). RV-arterial coupling was evaluated by combination of RV GLS and three proposed surrogates of RV afterload-pulmonary artery systolic pressure (PASP), pulmonary vascular resistance (PVR) and pulmonary artery compliance (PAC). 18-FDG positron emission tomography (PET) analysis was used to assess RV glucose uptake presented as SUVRV/LV. Follow-up time of this study was 25 months and the clinical end-point was defined as death or clinical deterioration.
Results: Coupling parameters (RV GLS/PASP, RV GLS/PVR and RV GLS*PAC) significantly correlated with RV function and standardized uptake value (SUVRV/LV). Patients who experienced a clinical end-point (n = 18) had a significantly worse coupling parameters at the baseline visit. RV GLS/PASP had the highest area under curve in predicting a clinical end-point and patients with a value higher than (-)0.29%/mmHg had significantly worse prognosis. It was also a statistically significant predictor of clinical end-point in multivariate analysis (adjusted R2 = 0.68; p < 0.001).
Conclusions: Coupling parameters are linked with RV hemodynamics and glucose metabolism in PAH. Combining CMR and hemodynamic measurements offers more comprehensive assessment of RV function required for prognostication of PAH patients.
Trial registration: NCT03688698, 09/26/2018, retrospectively registered; Protocol ID: 2017/25/N/NZ5/02689.
Keywords: Cardiovascular magnetic resonance; Coupling; Positron emission tomography; Primary pulmonary hypertension; Prognosis.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Galiè N, Humbert M, Vachiery JL, et al. ESC Scientific Document Group. Guidelines for the diagnosis and treatment of pulmonary hypertension: the task force for the diagnosis and treatment of pulmonary hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS), endorsed by the International Society of Heart and Lung Transplantation (ISHLT) Eur Heart J. 2016;37:67–119. doi: 10.1093/eurheartj/ehv317. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
