

Surgical management of empyema thoracis - experience of a decade in a tertiary care centre in India
- PMID: 33967415
- PMCID: PMC8079569
- DOI: 10.1007/s12055-020-01085-x
Surgical management of empyema thoracis - experience of a decade in a tertiary care centre in India
Abstract
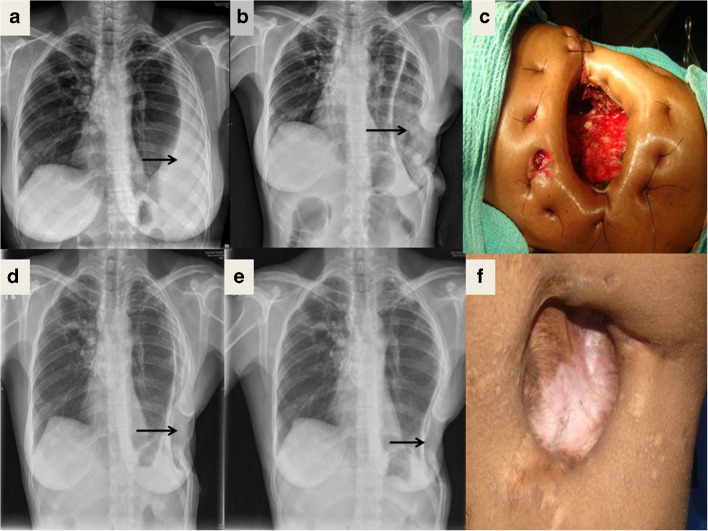
Introduction and purpose: Empyema thoracis (ET) is defined as the accumulation of pus in the pleural cavity. Early stages of ET are treated medically and the late stages surgically. Decortication, thoracoplasty, window procedure (Eloesser flap procedure) and rib resections are the open surgical procedures executed. There are no strict guidelines available in developing nations to guide surgical decision-making, as to which procedure is to be followed.
Methods: Details of all adult patients treated surgically for ET, between the years 2009 and 2019, and maintained in a live database in our institute, were retrieved and analysed. Medically managed patients were excluded.
Results: There were 437 patients in the study. The average age was 38 years. There was right side preponderance with a male:female ratio of 5:1. Tuberculosis was the commonest aetiology identified in 248 (57%) patients and diabetes was the commonest co-morbidity present in 97 (22%) patients. There was a higher incidence of a window procedure (WP) in tubercular patients 145 (59%). Only 26 (14%) of the non-tubercular patients underwent a WP. Post-operative complications were persistent air leak in 12 (6%) patients and premature closure of a window in 7 (4%) patients. There were 4 (0.9%) post-operative mortalities.
Conclusion: Surgical management of late stages of ET provides good results with minimal morbidity and mortality. In developing nations like India, the high incidence of tuberculosis and late presentations make the surgical management difficult and the strategies different from those in developed nations. No clear guidelines exist for the surgical management of ET in developing nations. There is a need for a consensus on the surgical management of empyema in such countries.
Keywords: Decortication; Empyema; Rib resection; Thoracoplasty; Tuberculosis; Window procedure.
© Indian Association of Cardiovascular-Thoracic Surgeons 2021.
Conflict of interest statement
Conflict of interestThe authors declare that there is no conflict of interest.
Figures




References
-
- Frank S, Pedro DN, Scott JS. Benign pleural diseases: empyema thoracis. In: Sabiston and Spencer surgery of the chest, 9th Edition. Elsevier Company; 2015:467–75.
-
- Light RW. Parapneumonic effusions and empyema. In: Rhyner S, Winter N, Koleth J, editors. Pleural diseases. 5. Philadelphia: Lippincott Williams and Wilkins; 2007. pp. 179–210.
-
- Andrews NC, Parker EF, Shaw RR, Wilson NJ, Webb WR. Management of nontuberculous empyema. Am Rev Respir Dis. 1962;85:935–936.
LinkOut - more resources
Full Text Sources
Other Literature Sources