

No Efficacy of the Combination of Lopinavir/Ritonavir Plus Hydroxychloroquine Versus Standard of Care in Patients Hospitalized With COVID-19: A Non-Randomized Comparison
- PMID: 33967755
- PMCID: PMC8100580
- DOI: 10.3389/fphar.2021.621676
No Efficacy of the Combination of Lopinavir/Ritonavir Plus Hydroxychloroquine Versus Standard of Care in Patients Hospitalized With COVID-19: A Non-Randomized Comparison
Abstract
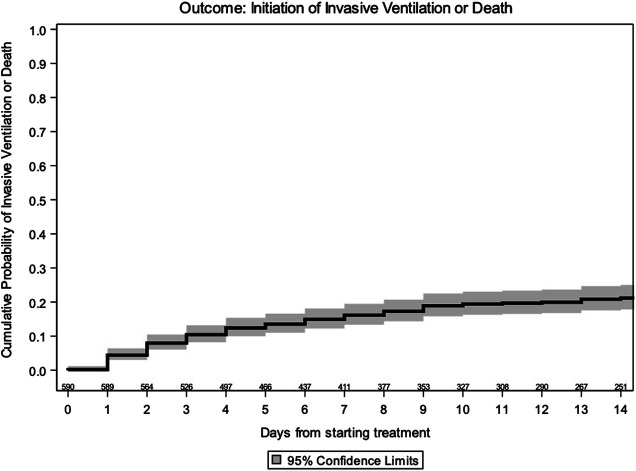
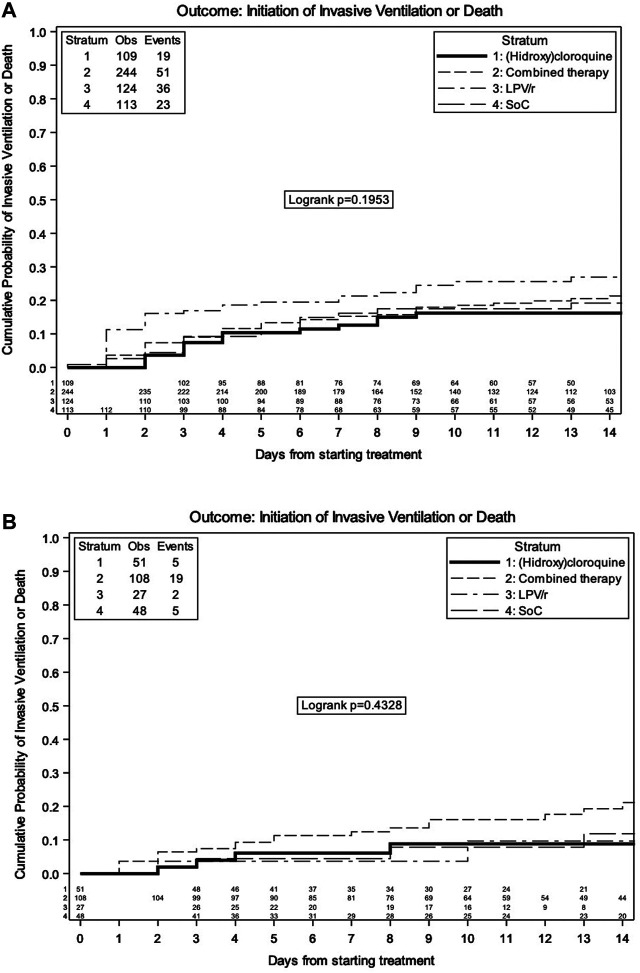
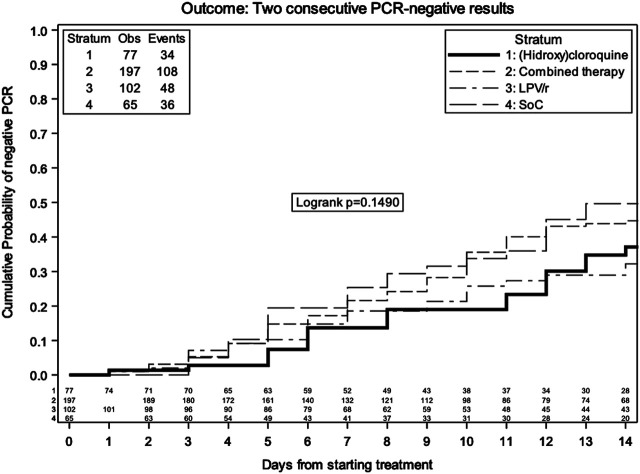
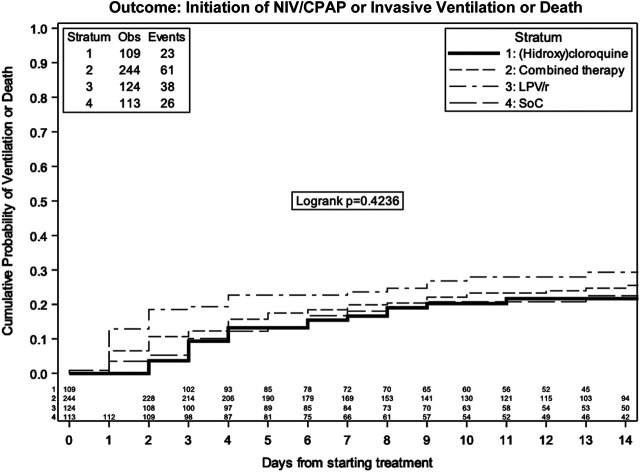
Objectives: No specific treatment has been approved for COVID-19. Lopinavir/ritonavir (LPV/r) and hydroxychloroquine (HCQ) have been used with poor results, and a trial showed advantages of combined antiviral therapy vs. single antivirals. The aim of the study was to assess the effectiveness of the combination of antivirals (LPV/r and HCQ) or their single use in COVID-19 hospitalized patients vs. standard of care (SoC). Methods: Patients ≥18 years with SARS-CoV-2 infection, defined as positive RT-PCR from nasal/oropharyngeal (NP/OP) swab or positive serology, admitted at L. Spallanzani Institute (Italy) were included. Primary endpoint: time to invasive ventilation/death. Secondary endpoint: time to two consecutive negative SARS-CoV-2 PCRs in NP/OP swabs. In order to control for measured confounders, a marginal Cox regression model with inverse probability weights was used. Results: A total of 590 patients were included in the analysis: 36.3% female, 64 years (IQR 51-76), and 91% with pneumonia. Cumulative probability of invasive ventilation/death at 14 days was 21.2% (95% CI 17.6, 24.7), without difference between SOC, LPV/r, hydroxychloroquine, HCQ + LPV/r, and SoC. The risk of invasive ventilation/death in the groups appeared to vary by baseline ratio of arterial oxygen partial pressure to fractional inspired oxygen (PaO2/FiO2). Overall cumulative probability of confirmed negative nasopharyngeal swabs at 14 days was 44.4% (95% CI 38.9, 49.9), without difference between groups. Conclusion: In this retrospective analysis, we found no difference in the rate of invasive ventilation/death or viral shedding by different strategies, as in randomized trials performed to date. Moreover, even the combination HCQ + LPV/r did not show advantages vs. SoC.
Keywords: SARS-CoV-2; antivirals; drug repurposing; invasive ventilation; viral shedding.
Copyright © 2021 Gagliardini, Cozzi-Lepri, Mariano, Taglietti, Vergori, Abdeddaim, Di Gennaro, Mazzotta, Amendola, D’Offizi, Palmieri, Marchioni, Piselli, Agrati, Nicastri, Capobianchi, Petrosillo, Ippolito, Vaia, Girardi and Antinori.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- European Centre for Disease Prevention and Control (2020). Outbreak of novel coronavirus disease 2019 (COVID-19): increased transmission globally–fifth update. Stockholm, Sweden: ECDC; (Accessed March 2, 2020).
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous