

Geographical Latitude Remains as an Important Factor for the Prevalence of Some Myositis Autoantibodies: A Systematic Review
- PMID: 33968081
- PMCID: PMC8100663
- DOI: 10.3389/fimmu.2021.672008
Geographical Latitude Remains as an Important Factor for the Prevalence of Some Myositis Autoantibodies: A Systematic Review
Abstract
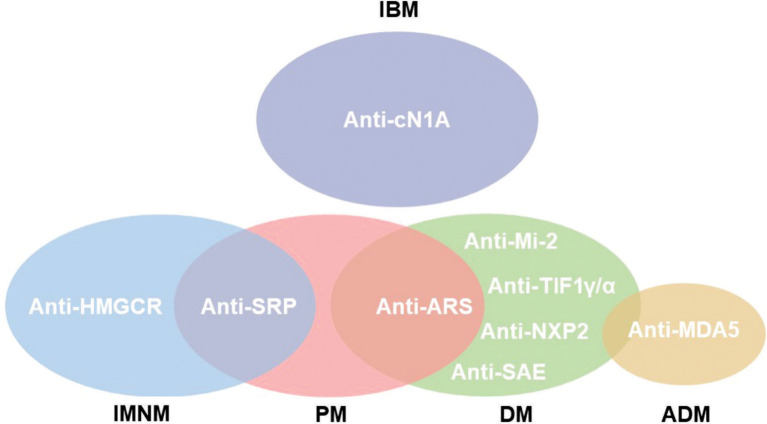
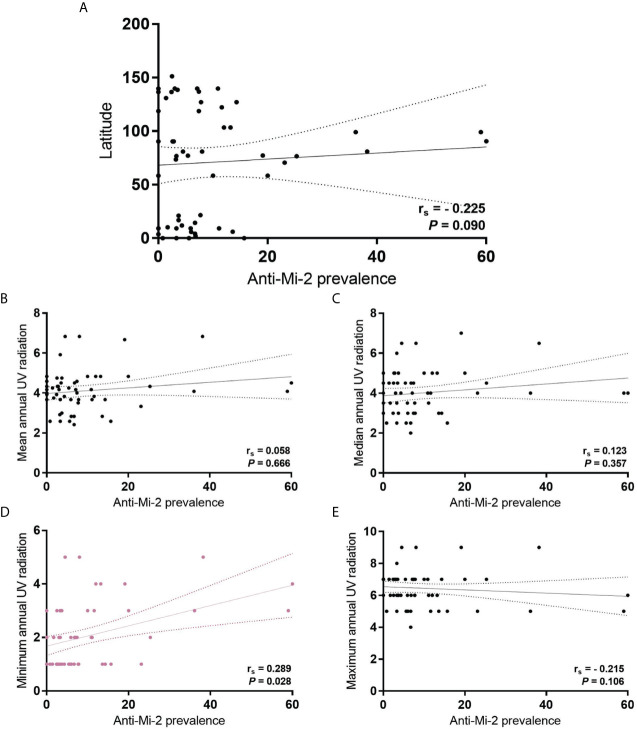
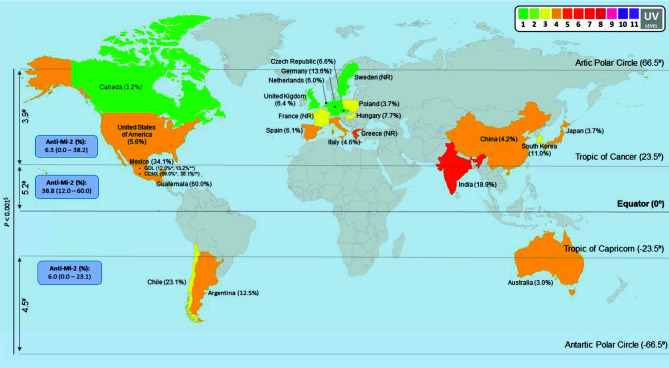
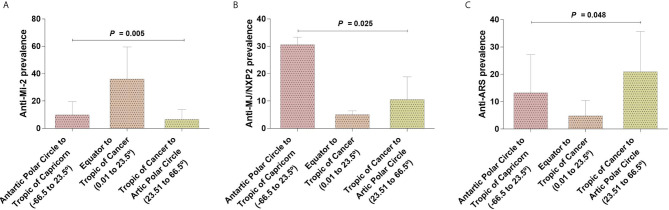
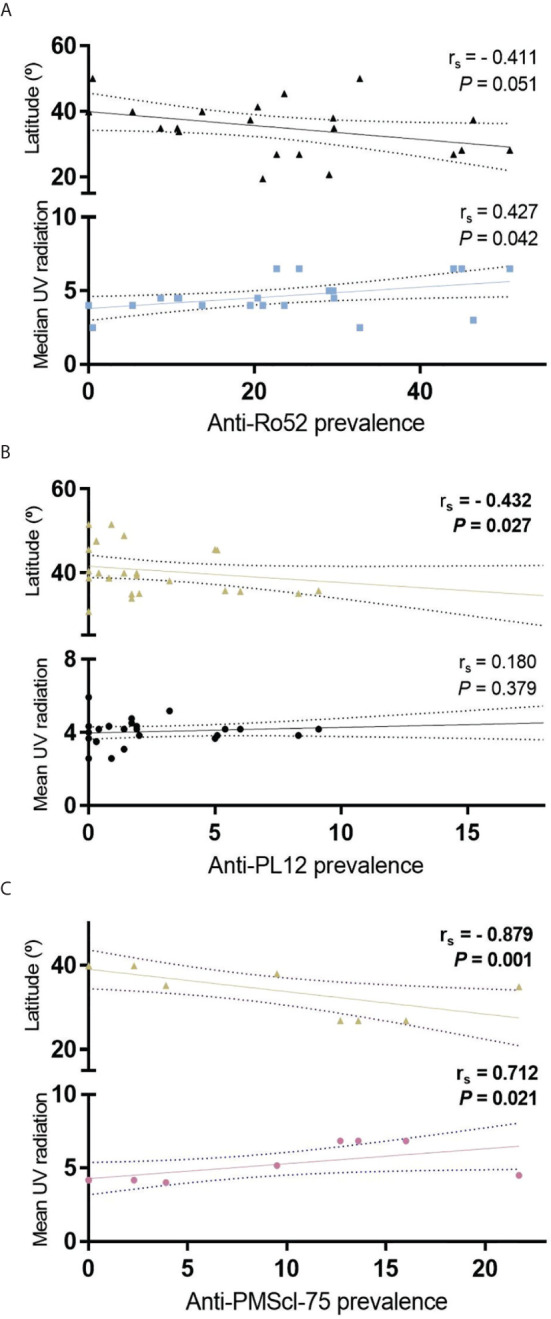
The idiopathic inflammatory myopathies (IIM) are characterized by muscular weakness, cutaneous manifestations, muscle damage revealed by increase of muscular enzymes, muscle biopsy, electromyography and changes on magnetic resonance imaging. However, the hallmark of these IIM, is the development of myositis specific antibodies (MSA) or myositis associated antibodies (MAA). The theories about their presence in the serum of IIM is not known. Some studies have suggested that some of these MSA, such as anti-Mi-2 increases according to the intensity of UV radiation. There is scarce information about the environmental factors that might contribute in order to be considered as triggering factors as UV radiation might be. In this review, we analyzed the reported prevalence of MSAs and MAAs regarding to their geographical location and the possible relation with UV radiation. We collected the prevalence data of fifteen MSA and thirteen MAA from 22 countries around the world and we were able to observe a difference in prevalence between countries and continents. We found differences in anti-PL7, anti-Ro52, anti-La and anti-Ku prevalence according to UV radiation level. Otherwise, we observed that anti-Mi-2 prevalence increases near to the Equator meanwhile anti-MJ/NXP2 and anti-ARS prevalence had an opposite behavior increasing their prevalence in the geographical locations farther to the Equator. Our results highlighted the importance to include the UV radiation and other environmental factors in IIM studies, in order to clarify its association with MSA and MAA prevalence as well as its possible role in the immunopathogenesis of these diseases.
Keywords: UV radiation; autoantibodies; idiopathic inflammatory myopathies (IIM); latitude; prevalence.
Copyright © 2021 Aguilar-Vazquez, Chavarria-Avila, Pizano-Martinez, Ramos-Hernandez, Andrade-Ortega, Rubio-Arellano and Vazquez-Del Mercado.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Myositis autoantibody profiles and their clinical associations in Greek patients with inflammatory myopathies.Clin Rheumatol. 2019 Jan;38(1):125-132. doi: 10.1007/s10067-018-4267-z. Epub 2018 Aug 25. Clin Rheumatol. 2019. PMID: 30145635
-
Frequency, mutual exclusivity and clinical associations of myositis autoantibodies in a combined European cohort of idiopathic inflammatory myopathy patients.J Autoimmun. 2019 Jul;101:48-55. doi: 10.1016/j.jaut.2019.04.001. Epub 2019 Apr 13. J Autoimmun. 2019. PMID: 30992170 Free PMC article.
-
Myositis-specific and myositis-associated autoantibodies in a large Indian cohort of inflammatory myositis.Semin Arthritis Rheum. 2021 Feb;51(1):113-120. doi: 10.1016/j.semarthrit.2020.10.014. Epub 2020 Dec 22. Semin Arthritis Rheum. 2021. PMID: 33360322
-
[Myositis specific autoantibodies as a new diagnostic criterion for idiopathic inflammatory myopathies].Neurol Neurochir Pol. 2000 Mar-Apr;34(2):339-47. Neurol Neurochir Pol. 2000. PMID: 10962726 Review. Polish.
-
Narrative review of autoantibodies in idiopathic inflammatory myopathies.Ann Transl Med. 2023 Apr 15;11(7):291. doi: 10.21037/atm-21-475. Epub 2021 Dec 10. Ann Transl Med. 2023. PMID: 37090051 Free PMC article. Review.
Cited by
-
Long Term Outcomes in Idiopathic Inflammatory Myositis: An Observational Epidemiologic Study over 15 Years.Mediterr J Rheumatol. 2023 Aug 28;34(4):513-524. doi: 10.31138/mjr.280823.lto. eCollection 2023 Dec. Mediterr J Rheumatol. 2023. PMID: 38282927 Free PMC article.
-
Autoantibodies in the pathogenesis of idiopathic inflammatory myopathies: Does the endoplasmic reticulum stress response have a role?Front Immunol. 2022 Sep 15;13:940122. doi: 10.3389/fimmu.2022.940122. eCollection 2022. Front Immunol. 2022. PMID: 36189221 Free PMC article. Review.
-
Incidence and prevalence of idiopathic inflammatory myopathies in Thailand from the Ministry of Public Health data analysis.Sci Rep. 2024 Sep 4;14(1):20646. doi: 10.1038/s41598-024-71633-7. Sci Rep. 2024. PMID: 39232120 Free PMC article.
-
Profile of specific and associated autoantibodies in patients with idiopathic inflammatory myopathies in a Colombian population.Front Med (Lausanne). 2022 Aug 15;9:954937. doi: 10.3389/fmed.2022.954937. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36045923 Free PMC article.
-
Integrating Machine Learning into Myositis Research: a Systematic Review.Clin Rev Allergy Immunol. 2025 Jul 8;68(1):62. doi: 10.1007/s12016-025-09076-9. Clin Rev Allergy Immunol. 2025. PMID: 40624382 Free PMC article. Review.
References
-
- Lundberg IE, Tjarnlund A, Bottai M, Werth VP, Pilkington C, Visser M, et al. . European League Against Rheumatism/American College of Rheumatology Classification Criteria for Adult and Juvenile Idiopathic Inflammatory Myopathies and Their Major Subgroups. Ann Rheum Dis (2017) 76(12):1955–64. 10.1136/annrheumdis-2017-211468 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical