

Changes in peri-ocular anatomy and physiology in pseudoexfoliation syndrome (Review)
- PMID: 33968180
- PMCID: PMC8097227
- DOI: 10.3892/etm.2021.10082
Changes in peri-ocular anatomy and physiology in pseudoexfoliation syndrome (Review)
Abstract
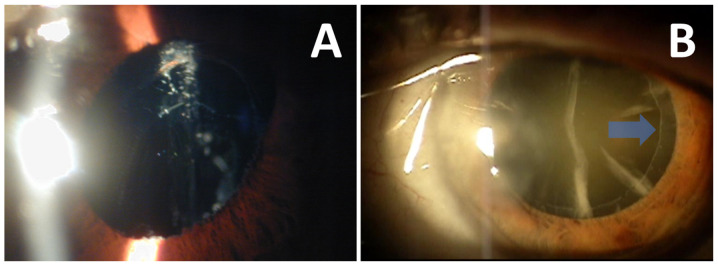
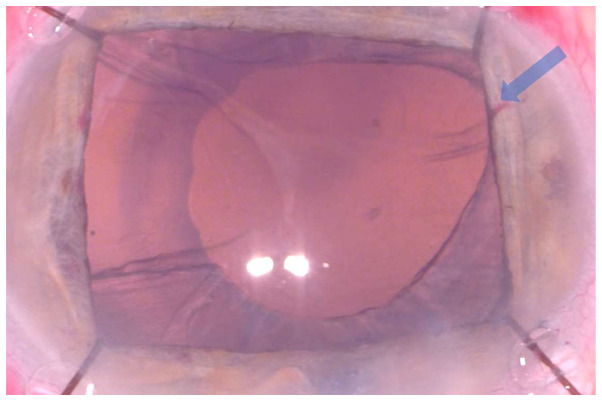
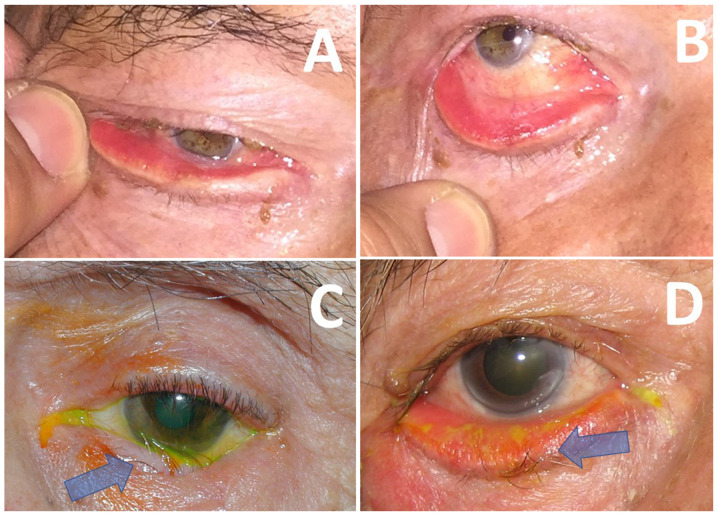
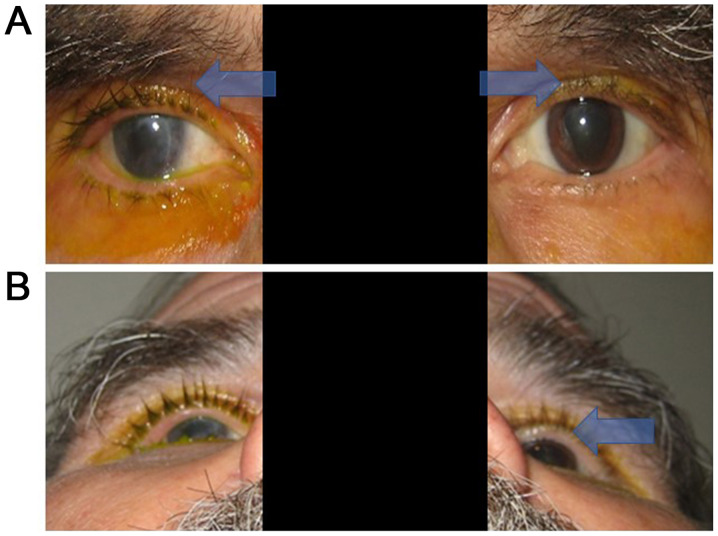
Pseudoexfoliation syndrome (PEX) is characterized by the deposition of proteinaceous material in the anterior ocular segment (resulting in ophthalmic pathologies such as glaucoma and increased risk of complications in cataract surgery), but also by several systemic manifestations. The involvement of peri-ocular tissues in PEX, including the eyelid skin, lacrimal gland, conjunctiva, orbital fat and vessels, as well as the optic nerve, has been reported by several previous studies. The peri-ocular effects of PEX include the development of eyelid laxity, conjunctival chalasis, tear film abnormalities, pronounced orbital fat atrophy in response to the administration of prostaglandin analogues in pseudoexfoliative glaucoma, deficient orbital vascular supply and biomechanical changes in both the eyeball and the optic nerve. These effects may have important clinical implications, including increased difficulty in cataract surgery, ocular surface disease and eyelid margin malpositions.
Keywords: eyelid; lacrimal; orbit; pseudoexfoliation; skin.
Copyright: © Detorakis et al.
Conflict of interest statement
DAS is the Editor in Chief for the journal, but had no personal involvement in the reviewing process, or any influence in terms of adjudicating on the final decision, for this article. The other authors declare that they have no competing interests.
Figures
Similar articles
-
Histopathological Analysis of Pseudoexfoliation Material in Ocular Surgeries: Clinical Implications.Diagnostics (Basel). 2024 Sep 30;14(19):2187. doi: 10.3390/diagnostics14192187. Diagnostics (Basel). 2024. PMID: 39410590 Free PMC article.
-
Novel protein constituents of pathological ocular pseudoexfoliation syndrome deposits identified with mass spectrometry.Mol Vis. 2018 Dec 28;24:801-817. eCollection 2018. Mol Vis. 2018. PMID: 30713420 Free PMC article.
-
Cataract Surgery and Possible Complications in Patients with Pseudoexfoliation Syndrome.Eurasian J Med. 2017 Feb;49(1):22-25. doi: 10.5152/eurasianjmed.2016.0060. Epub 2016 Aug 18. Eurasian J Med. 2017. PMID: 28416927 Free PMC article.
-
Pseudoexfoliation syndrome: pathological manifestations of relevance to intraocular surgery.Clin Exp Ophthalmol. 2004 Apr;32(2):199-210. doi: 10.1111/j.1442-9071.2004.00806.x. Clin Exp Ophthalmol. 2004. PMID: 15068440 Review.
-
[Pseudoexfoliation syndrome (PEX)--a systemic disorder].Klin Oczna. 2009;111(4-6):160-4. Klin Oczna. 2009. PMID: 19673450 Review. Polish.
Cited by
-
Pseudoexfoliation Syndrome-Clinical Characteristics of Most Common Cause of Secondary Glaucoma.J Clin Med. 2023 May 21;12(10):3580. doi: 10.3390/jcm12103580. J Clin Med. 2023. PMID: 37240686 Free PMC article. Review.
-
Implantation of a scleral fixated (Carlevale) EDOF IOL in aphakia.Am J Ophthalmol Case Rep. 2025 Jul 23;39:102391. doi: 10.1016/j.ajoc.2025.102391. eCollection 2025 Sep. Am J Ophthalmol Case Rep. 2025. PMID: 40761389 Free PMC article.
-
The Ocular Surface and the Anterior Segment of the Eye in the Pseudoexfoliation Syndrome: A Comprehensive Review.Int J Mol Sci. 2025 Jan 10;26(2):532. doi: 10.3390/ijms26020532. Int J Mol Sci. 2025. PMID: 39859251 Free PMC article. Review.
-
Histopathological Analysis of Pseudoexfoliation Material in Ocular Surgeries: Clinical Implications.Diagnostics (Basel). 2024 Sep 30;14(19):2187. doi: 10.3390/diagnostics14192187. Diagnostics (Basel). 2024. PMID: 39410590 Free PMC article.
References
-
- Elschnig A. A Detachment of the zonular lamellae in glassblowers. Klin Monatsbl Augenheilkd. 1922;69:732–734.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources