

Device closure of fistula from left lower pulmonary artery to left atrium using a vascular plug: A case report
- PMID: 33968310
- PMCID: PMC8069520
- DOI: 10.4330/wjc.v13.i4.111
Device closure of fistula from left lower pulmonary artery to left atrium using a vascular plug: A case report
Abstract
Background: Pulmonary artery-to-left atrial fistula is a variant of pulmonary arteriovenous fistula and is a developmental anomaly. Delayed presentation, cyanosis and effort intolerance are some of the important features. The diagnosis is confirmed by computed tomography or pulmonary artery angiography. Catheter-based closure is preferred to surgery.
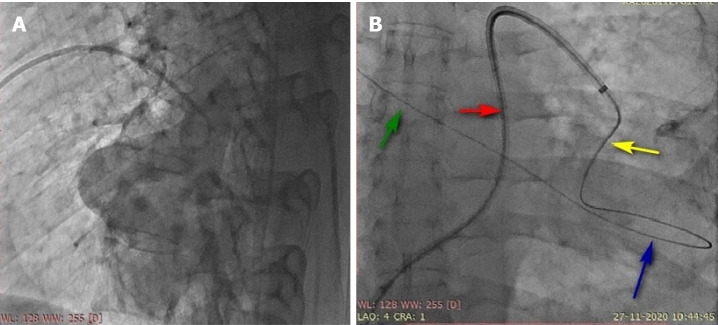
Case summary: Left pulmonary artery-to-left atrial fistula is rare. A 40-year-old male presented with effort intolerance, central cyanosis, and recurrent seizures. He had a large and highly tortuous left pulmonary artery-to-left atrial fistula associated with a large aneurysmal sac in the course. Catheter-based closure was performed using a vascular plug.
Conclusion: Left pulmonary artery-to-left atrial fistula is relatively uncommon compared to right pulmonary artery-to-left atrial fistula. Percutaneous closure by either a transeptal technique or guide wire insertion into the pulmonary vein through the pulmonary artery is preferred. The need for an arteriovenous loop depends on the tortuosity of the course of the fistula and the size of the device to be implanted because a larger device needs a larger sheath, necessitating firm guide wire support to facilitate negotiation of the stiff combination of the delivery sheath and dilator.
Keywords: Case report; Catheter-based; Fistula; Hemangioma; Left atrium; Pulmonary artery; Vascular plug.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflicts of interests or financial disclosures relevant to this manuscript.
Figures


References
-
- Mongé MC, Russell HM, Popescu AR, Robinson JD. Right pulmonary artery to left atrial fistula in a neonate: case report and review of the literature. World J Pediatr Congenit Heart Surg. 2014;5:306–310. - PubMed
-
- Jimenez M, Fournier A, Choussat A. Pulmonary artery to the left atrium fistula as an unusual cause of cyanosis in the newborn. Pediatr Cardiol. 1989;10:216–220. - PubMed
-
- Sivakumar K, Sean DR. Pulmonary artery to left atrial fistula: haemodynamic changes traced from fetus to infancy until its interventional closure. Cardiol Young. 2018;28:1154–1156. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
