

Review
doi: 10.1002/cld.1047.
eCollection 2021 Apr.
Pathology of Cholangiocarcinoma and Combined Hepatocellular-Cholangiocarcinoma
Affiliations
- PMID: 33968385
- PMCID: PMC8087927
- DOI: 10.1002/cld.1047
Item in Clipboard
Review
Pathology of Cholangiocarcinoma and Combined Hepatocellular-Cholangiocarcinoma
Clin Liver Dis (Hoboken).
.
No abstract available
Figures

iCC, corresponding to the small‐duct type. Tumor forms a well‐defined peripheral subcapsular mass. Note the nodularity of the background liver, indicating fibrosis secondary to chronic liver disease.

iCC, large‐duct type. Tumor has a mixed periductal (arrows) and mass‐forming (arrowhead) pattern.
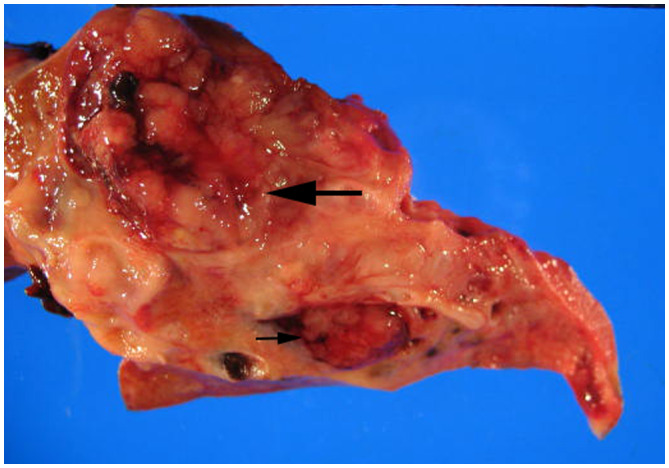
pCC. Tumor has an intraductal (small arrow) and mixed intraductal‐periductal (large arrow) infiltrating pattern.

(A) Tubular (acinar) pattern of CC with typical desmoplastic stromal response. (B) CC with mixed acinar (right) and sarcomatoid (left) patterns. (C) Characteristic cholangiolar pattern for a small‐duct CC, with focal pleomorphic cytological features (arrows). (D) CC with a cholangiolar pattern in a core biopsy. A metastasis would need to be excluded, such as from a breast primary. (E) CC arising from a large intrahepatic duct, with invasive tumor (CC) and HG BilIN. (F) IPN characterized by a papillary proliferation in a dilated duct. DW is seen at the periphery.

Hilar CC arising in the setting of PSC. Tumor is well differentiated with infiltrating glands containing mucinous epithelium. A cluster of benign periductal glands is present (arrow), and the duct lumen (D) is markedly narrowed.

HCC‐CC, with HCC and CC components.
References
-
- Nakanuma Y, Klimstra DS, Komuta M, et al. Intrahepatic cholangiocarcinoma. In: WHO Classification of Tumors: Digestive System Tumors. 5th ed. Lyon, France: IARC Press; 2019:254‐262.
-
- Roa JC, Adsay NV, Arola J, et al. Carcinoma of the extrahepatic bile ducts. WHO classification of tumors: Digestive system tumors, 5th edn. Lyon, France: IARC Press; 2019:289‐291.
-
- Bergquist A, Seth E. Epidemiology of cholangiocarcinoma. Best Pract Res Clin Gastroenterol 2015;29:221‐232. - PubMed
-
- Abu‐Wasel B, Keough V, Renfrew PD, et al. Biliary stent therapy for dominant strictures in patients affected by primary sclerosing cholangitis. Pathobiology 2013;80:182‐193. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
