

Systematic Review and Meta-Analysis of Diagnostic Agreement in Suspected TIA
- PMID: 33968473
- PMCID: PMC8101306
- DOI: 10.1212/CPJ.0000000000000830
Systematic Review and Meta-Analysis of Diagnostic Agreement in Suspected TIA
Abstract
Objective: To determine the interrater variability for TIA diagnostic agreement among expert clinicians (neurologists/stroke physicians), administrative data, and nonspecialists.
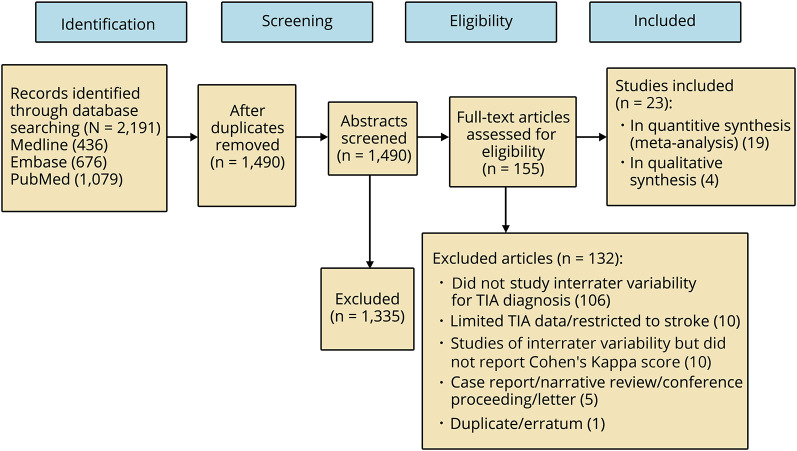
Methods: We performed a meta-analysis of studies from January 1984 to January 2019 using MEDLINE, EMBASE, and PubMed. Two reviewers independently screened for eligible studies and extracted interrater variability measurements using Cohen's kappa scores to assess diagnostic agreement.
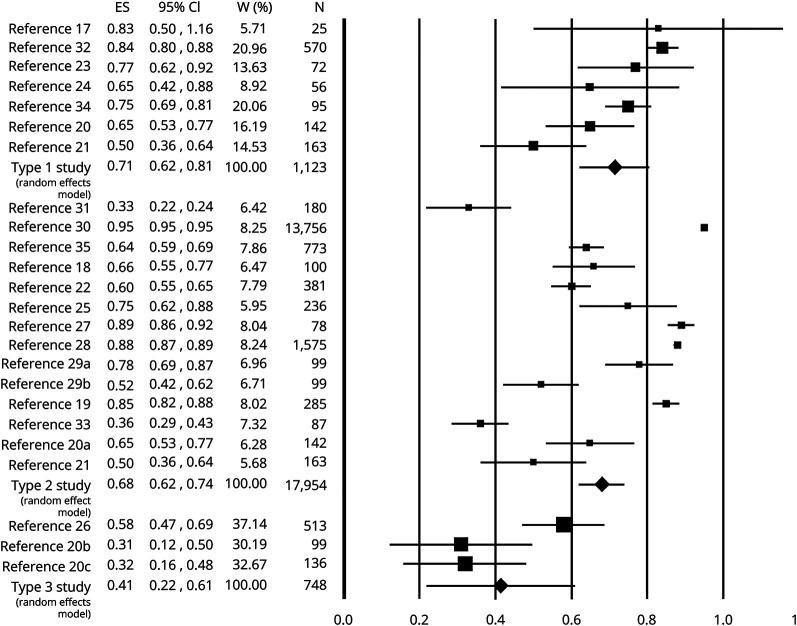
Results: Nineteen original studies consisting of 19,421 patients were included. Expert clinicians demonstrate good agreement for TIA diagnosis (κ = 0.71, 95% confidence interval [CI] = 0.62-0.81). Interrater variability between clinicians' TIA diagnosis and administrative data also demonstrated good agreement (κ = 0.68, 95% CI = 0.62-0.74). There was moderate agreement (κ = 0.41, 95% CI = 0.22-0.61) between referring clinicians and clinicians at TIA clinics receiving the referrals. Sixty percent of 748 patient referrals to TIA clinics were TIA mimics.
Conclusions: Overall agreement between expert clinicians was good for TIA diagnosis, although variation still existed for a sizeable proportion of cases. Diagnostic agreement for TIA decreased among nonspecialists. The substantial number of patients being referred to TIA clinics with other (often neurologic) diagnoses was large, suggesting that clinicians, who are proficient in managing TIAs and their mimics, should run TIA clinics.
© 2020 American Academy of Neurology.
Figures
Similar articles
-
Frequent inaccuracies in ABCD2 scoring in non-stroke specialists' referrals to a daily Rapid Access Stroke Prevention service.J Neurol Sci. 2013 Sep 15;332(1-2):30-4. doi: 10.1016/j.jns.2013.05.030. Epub 2013 Jul 17. J Neurol Sci. 2013. PMID: 23871489
-
Risk of Subsequent Stroke Among Patients Receiving Outpatient vs Inpatient Care for Transient Ischemic Attack: A Systematic Review and Meta-analysis.JAMA Netw Open. 2022 Jan 4;5(1):e2136644. doi: 10.1001/jamanetworkopen.2021.36644. JAMA Netw Open. 2022. PMID: 34985520 Free PMC article.
-
Validation of ABCD2 scores ascertained by referring clinicians: a retrospective transient ischaemic attack clinic cohort study.Emerg Med J. 2016 Aug;33(8):543-7. doi: 10.1136/emermed-2015-205519. Epub 2016 Apr 7. Emerg Med J. 2016. PMID: 27056830
-
Agreement regarding diagnosis of transient ischemic attack fairly low among stroke-trained neurologists.Stroke. 2010 Jul;41(7):1367-70. doi: 10.1161/STROKEAHA.109.577650. Epub 2010 May 27. Stroke. 2010. PMID: 20508192
-
Interrater agreement in dementia diagnosis: A systematic review and meta-analysis.Int J Geriatr Psychiatry. 2021 Aug;36(8):1127-1147. doi: 10.1002/gps.5499. Epub 2021 May 3. Int J Geriatr Psychiatry. 2021. PMID: 33942363
Cited by
-
Comparison of Dual Antiplatelet Therapies for Minor, Nondisabling, Acute Ischemic Stroke: A Bayesian Network Meta-Analysis.JAMA Netw Open. 2024 May 1;7(5):e2411735. doi: 10.1001/jamanetworkopen.2024.11735. JAMA Netw Open. 2024. PMID: 38753327 Free PMC article.
-
European Stroke Organisation (ESO) guidelines on management of transient ischaemic attack.Eur Stroke J. 2021 Jun;6(2):CLXIII-CLXXXVI. doi: 10.1177/2396987321992905. Epub 2021 Mar 16. Eur Stroke J. 2021. PMID: 34414299 Free PMC article.
-
Hemodynamic analysis of non-stenotic middle cerebral artery in patients with cerebral ischemia based on 4D flow MRI.Front Neurosci. 2025 Jul 10;19:1502987. doi: 10.3389/fnins.2025.1502987. eCollection 2025. Front Neurosci. 2025. PMID: 40708689 Free PMC article.
References
-
- Johnston SC, Rothwell PM, Nguyen-Huynh MN, et al. . Validation and refinement of scores to predict very early stroke risk after transient ischaemic attack. Lancet 2007;369:283–292. - PubMed
-
- Prabhakaran S, Silver AJ, Warrior L, McClenathan B, Lee VH. Misdiagnosis of transient ischemic attacks in the emergency room. Cerebrovasc Dis 2008;26:630–635. - PubMed
-
- Rothwell PM, Giles MF, Chandratheva A, et al. . Effect of urgent treatment of transient ischaemic attack and minor stroke on early recurrent stroke (EXPRESS study): a prospective population-based sequential comparison. Lancet 2007;370:1432–1442. - PubMed
Publication types
LinkOut - more resources
Full Text Sources