

Initial Experience With a Full Endoscopic Facet Fusion in Combination With Endoscopic Interbody Fusion
- PMID: 33968535
- PMCID: PMC8101511
- DOI: 10.7759/cureus.14327
Initial Experience With a Full Endoscopic Facet Fusion in Combination With Endoscopic Interbody Fusion
Abstract
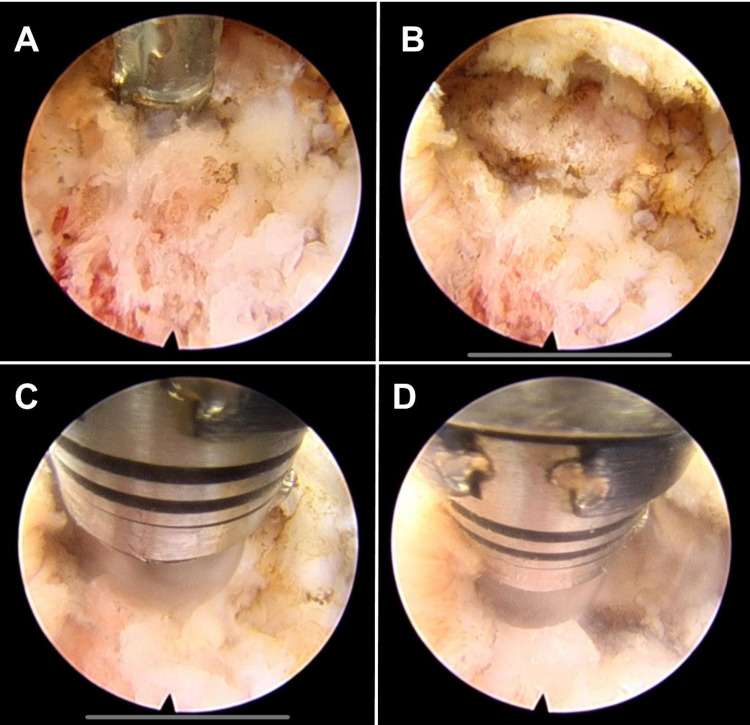
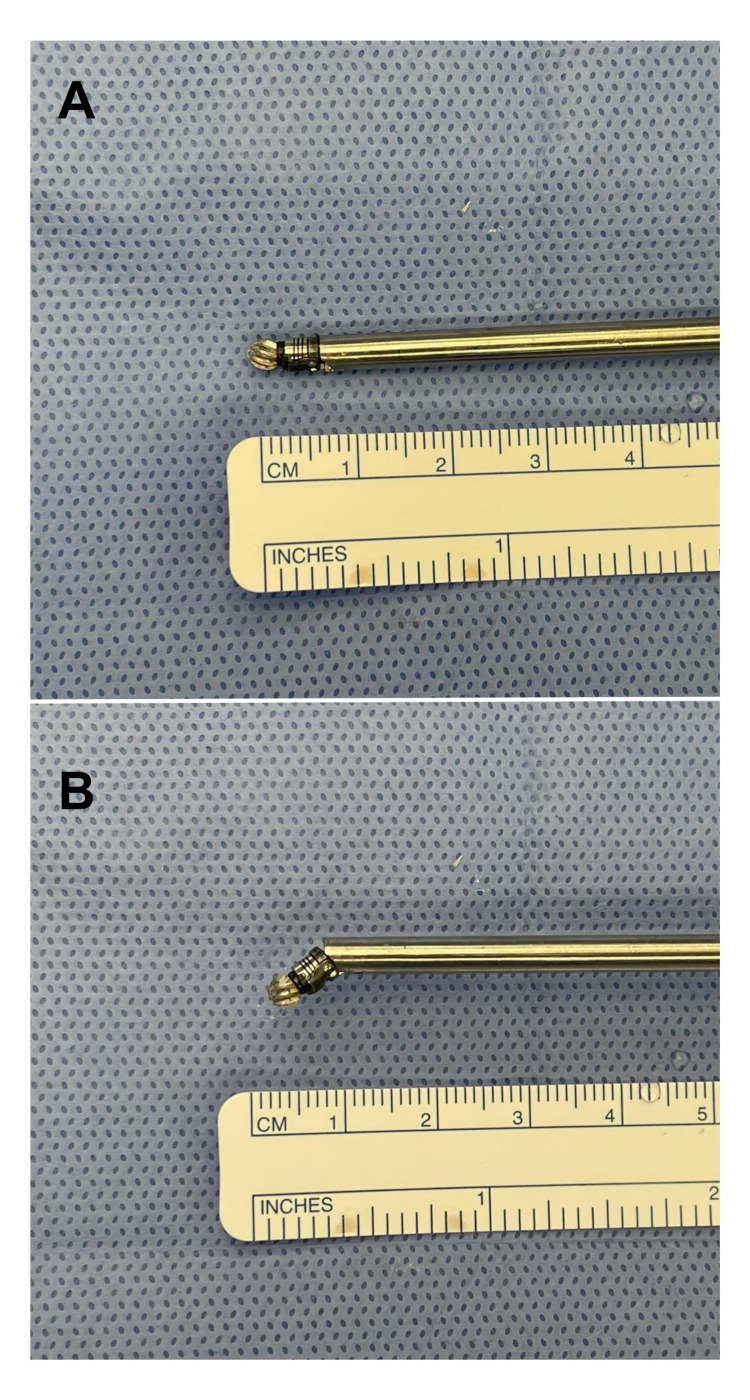
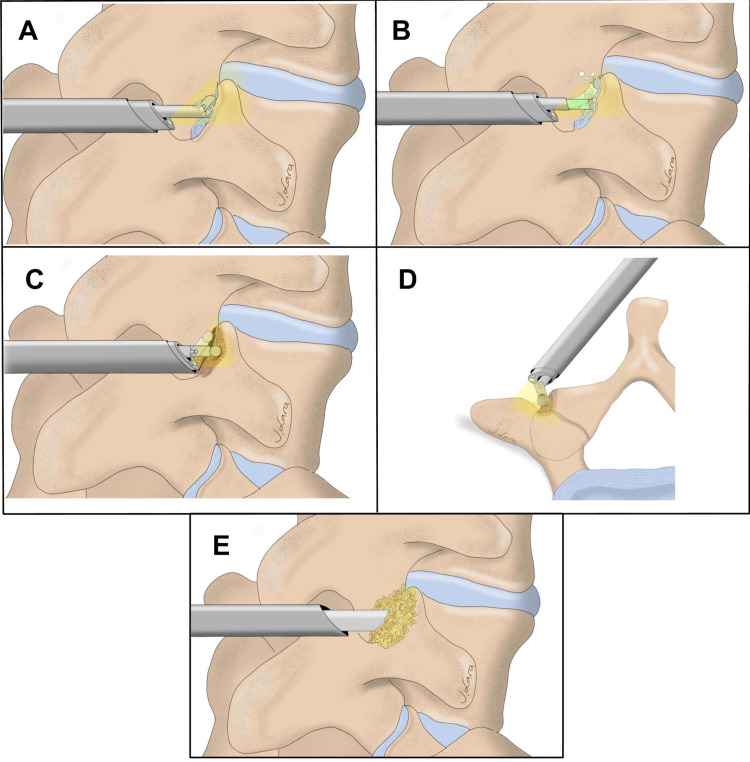
Background Facet fusion has been described in open and minimally invasive approaches to promote fusion. Our objective is to describe the technique of an endoscopic facet decortication and allograft placement as an adjunct to an interbody fusion. Methodology This was a descriptive analysis of patients who underwent endoscopic interbody fusion combined with facet fusion and percutaneous screw placement. General demographics, clinical presentation, length of stay, follow-up, and outcome were gathered. The technique involves endoscopic access to the Kambin's triangle, discectomy/endplate preparation, expandable cage/allograft insertion, and percutaneous pedicle screw placement. A midline incision was performed, and the endoscope was advanced over the facet joints at the desired level. After removing the soft tissue with grasping forceps, cautery was used to disrupt the facet capsule. An articulating high-speed bur was used to drill inside and over the dorsal surface of the joint. Finally, allograft chips were placed through the endoscope cannula. Results From May 2019 to December 2019, four patients underwent endoscopic interbody fusion. All were female, with a mean age of 67.5 years (SD: 12.7). All had chronic low back pain and radiculopathy associated with Grade 1 spondylolisthesis. Two (50%) of the patients underwent two-level fusion. The median hospital stay was two days. Two (50%) reported improvement of both low back and radiculopathy symptoms. None of the patients had a significant complication or required reoperation in eight months' mean follow-up. Conclusions Facet decortication and allograft placement are feasible using an endoscopic approach in conjunction with interbody fusion.
Keywords: endoscopy; lumbar degenerative disease; lumbar fusion; minimally invasive spine.
Copyright © 2021, Lara-Reyna et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Endoscopic minimally invasive transforaminal interbody fusion without general anesthesia: initial clinical experience with 1-year follow-up.Neurosurg Focus. 2016 Feb;40(2):E13. doi: 10.3171/2015.11.FOCUS15435. Neurosurg Focus. 2016. PMID: 26828882
-
Percutaneous Lumbar Interbody Fusion With an Expandable Titanium Cage Through Kambin's Triangle: A Case Series With Initial Clinical and Radiographic Results.Int J Spine Surg. 2021 Dec;15(6):1133-1141. doi: 10.14444/8144. Int J Spine Surg. 2021. PMID: 35086870 Free PMC article.
-
Minimally Invasive Transforaminal Lumbar Interbody Fusion (MI-TLIF): A Video Technique Guide.JBJS Essent Surg Tech. 2023 Oct 4;13(4):e21.00065. doi: 10.2106/JBJS.ST.21.00065. eCollection 2023 Oct-Dec. JBJS Essent Surg Tech. 2023. PMID: 38380431 Free PMC article.
-
[Facet Fixation Combined with Lumbar Interbody Fusion: Comparative Analysis of Clinical Experience and A New Method of Surgical Treatment of Patients with Lumbar Degenerative Diseases].Vestn Ross Akad Med Nauk. 2016;71(5):375-84. doi: 10.15690/vramn738. Vestn Ross Akad Med Nauk. 2016. PMID: 29297667 Russian.
-
The History of and Controversy over Kambin's Triangle: A Historical Analysis of the Lumbar Transforaminal Corridor for Endoscopic and Surgical Approaches.World Neurosurg. 2019 Mar;123:402-408. doi: 10.1016/j.wneu.2018.10.221. Epub 2018 Nov 9. World Neurosurg. 2019. PMID: 30415041 Review.
References
-
- Dr. Russell A. Hibbs: pioneer of spinal fusion. Miller DJ, Vitale MG. Spine (Phila Pa 1976) 2015;40:1311–1313. - PubMed
-
- Posterolateral fusion of the lumbar and lumbosacral spine. Watkins MB. https://insights.ovid.com/pubmed?pmid=14039825. J Bone Joint Surg Am. 1953;35:1014–1018. - PubMed
-
- Minimally invasive lumbar fusion. Foley KT, Holly LT, Schwender JD. Spine. 2003;28:26. - PubMed
-
- A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. Charlson ME, Pompei P, Ales KL, MacKenzie CR. J Chronic Dis. 1987;40:373–383. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources