

Intraoperative Ultrasound-Assisted Extent of Resection Assessment in Pediatric Neurosurgical Oncology
- PMID: 33968768
- PMCID: PMC8097032
- DOI: 10.3389/fonc.2021.660805
Intraoperative Ultrasound-Assisted Extent of Resection Assessment in Pediatric Neurosurgical Oncology
Abstract
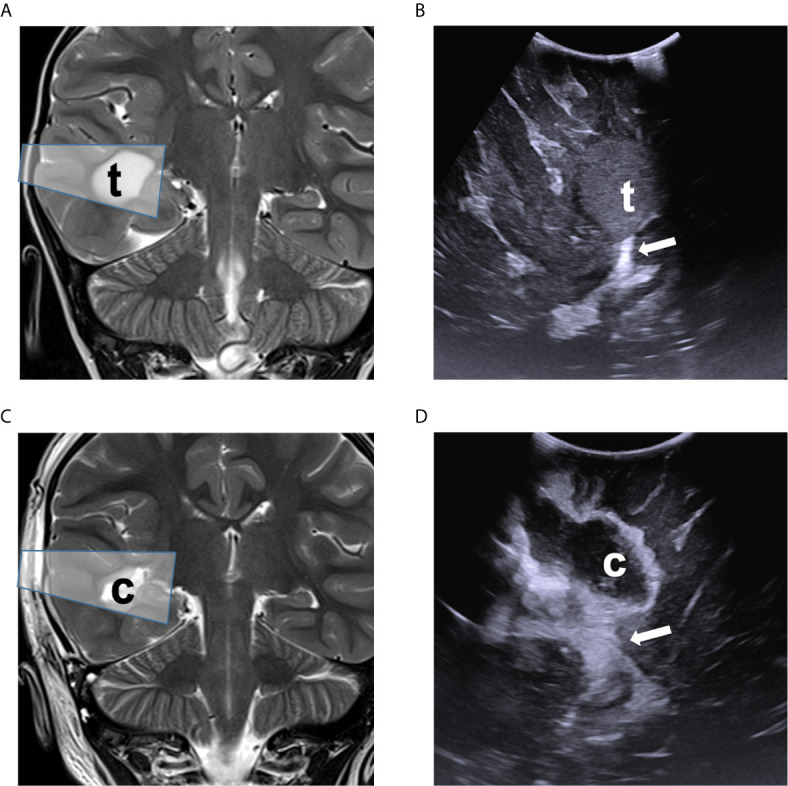
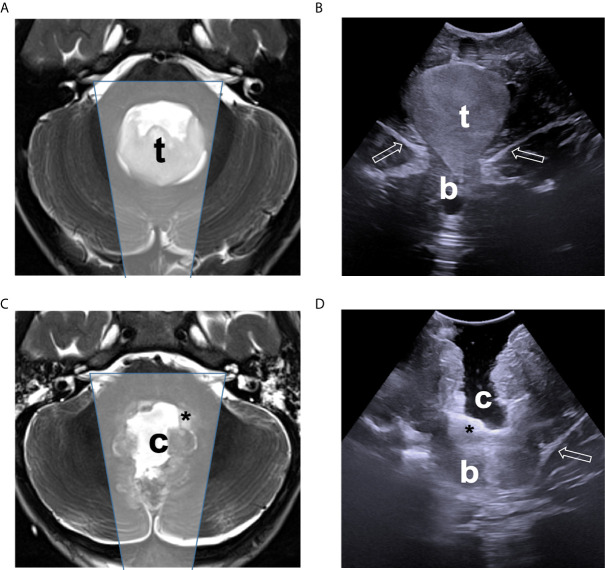
Central nervous system tumors represent the most frequent solid malignancy in the pediatric population. Maximal safe surgical resection is a mainstay of treatment, with significant prognostic impact for the majority of histotypes. Intraoperative ultrasound (ioUS) is a widely available tool in neurosurgery to assist in intracerebral disease resection. Despite technical caveats, preliminary experiences suggest a satisfactory predictive ability, when compared to magnetic resonance imaging (MRI) studies. Most of the available evidence on ioUS applications in brain tumors derive from adult series, a scenario that might not be representative of the pediatric population. We present our preliminary experience comparing ioUS-assisted resection assessment to early post-operative MRI findings in 154 consecutive brain tumor resections at our pediatric neurosurgical unit. A high concordance was observed between ioUS and post-operative MRI. Overall ioUS demonstrated a positive predictive value of 98%, a negative predictive value of 92% in assessing the presence of tumor residue compared to postoperative MRI. Overall, sensibility and specificity were 86% and 99%, respectively. On a multivariate analysis, the only variable significantly associated to unexpected tumor residue on postoperative MRI was histology. Tumor location, patient positioning during surgery, age and initial tumor volume were not significantly associated with ioUS predictive ability. Our data suggest a very good predictive value of ioUS in brain tumor resective procedures in children. Low-grade glioma, high-grade glioma and craniopharyngioma might represent a setting deserving specific endeavours in order to improve intraoperative extent of resection assessment ability.
Keywords: brain tumor; children; extent of resection; intraoperative ultrasound; neurosurgical oncology.
Copyright © 2021 Carai, De Benedictis, Calloni, Onorini, Paternò, Randi, Colafati, Mastronuzzi and Marras.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Chacko AG, Kumar NKS, Chacko G, Athyal R, Rajshekhar V, Unsgaard G. Intraoperative ultrasound in determining the extent of resection of parenchymal brain tumours - A comparative study with computed tomography and histopathology. Acta Neurochirurgica (2003) 145:743–8. 10.1007/s00701-003-0009-2 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources