

The Prenatal Origin of Childhood Leukemia: Potential Applications for Epidemiology and Newborn Screening
- PMID: 33968846
- PMCID: PMC8102903
- DOI: 10.3389/fped.2021.639479
The Prenatal Origin of Childhood Leukemia: Potential Applications for Epidemiology and Newborn Screening
Abstract
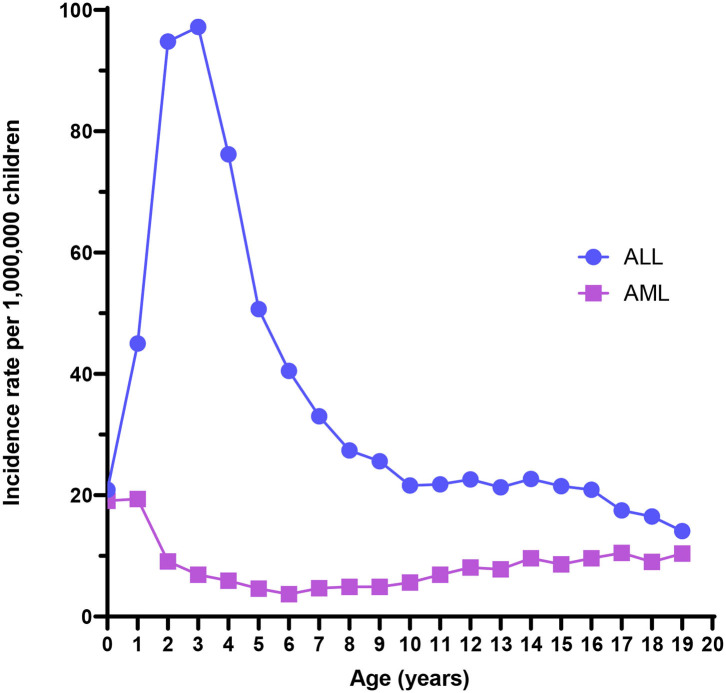
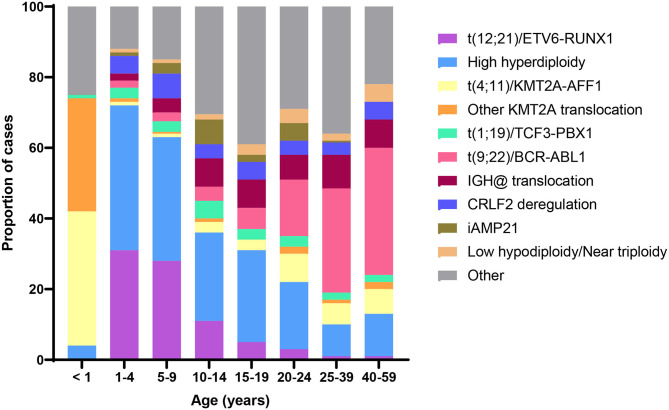
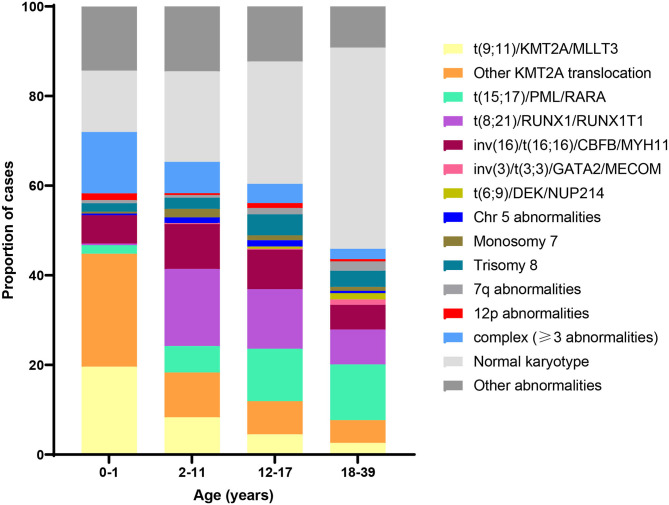
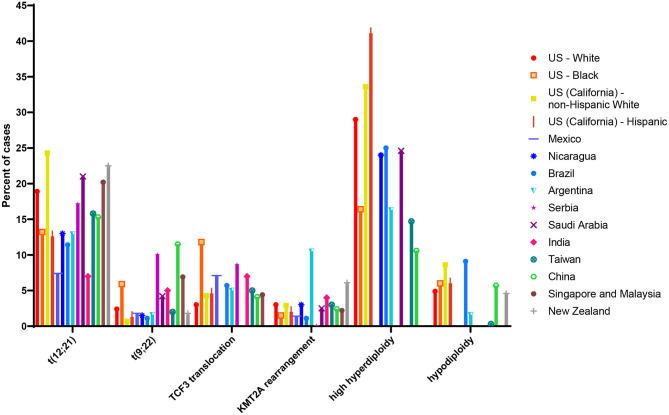
Childhood leukemias are heterogeneous diseases with widely differing incident rates worldwide. As circulating tumors, childhood acute leukemias are uniquely accessible, and their natural history has been described in greater detail than for solid tumors. For several decades, it has been apparent that most cases of childhood acute lymphoblastic leukemia (ALL) and acute myeloid leukemia (AML) initiate in utero. Circumstantial evidence in support of this contention includes the young age of onset and high rate of concordance among identical twins. "Backtracking" of leukemic somatic mutations, particularly gene translocations, to cord blood and dried blood spots collected during the perinatal period has provided molecular proof of prenatal leukemogenesis. Detection of a patient's leukemia translocation in easily accessible birth samples, such as dried blood spots, is straightforward with the knowledge of their idiosyncratic breakpoints. However, to translate these findings into population-based screening and leukemia prevention requires novel methods able to detect translocations at all possible breakpoints when present in a low frequency of cells. Several studies have attempted to screen for leukemic translocations, mainly the common ETV6-RUNX1 translocation, in cord blood samples from healthy children. Most studies have reported finding translocations in healthy children, but estimates of prevalence have varied widely and greatly exceed the incidence of leukemia, leading to concerns that technical artifact or contamination produced an artificially inflated estimate of translocation prevalence at birth. New generation techniques that capture the presence of these translocations at birth have the potential to vastly increase our understanding of the epidemiology of acute leukemias. For instance, if leukemic translocations are present at birth in a far higher proportion of children than eventually develop acute leukemia, what are the exposures and somatic molecular events that lead to disease? And could children with translocations present at birth be targeted for prevention of disease? These questions must be answered before large-scale newborn screening for leukemia can occur as a public health initiative. Here, we review the literature regarding backtracking of acute leukemias and the prevalence of leukemic translocations at birth. We further suggest an agenda for epidemiologic research using new tools for population screening of leukemic translocations.
Keywords: childhood leukemia; epidemiology; leukemia; newborns; screening; translocation.
Copyright © 2021 Marcotte, Spector, Mendes-de-Almeida and Nelson.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Surveillance Epidemiology and End Results (SEER) Program, SEER*Stat Database: Incidence - SEER 18 Regs Research Data + Hurricane Katrina Impacted Louisiana Cases Nov 2016 Sub (2000-2014) <Katrina/Rita Population Adjustment> - Linked To County Attributes - Total U.S., 1969-2015 Counties. Bethesda, MD: Naitonal Cancer Institute.
-
- Greaves M. Pre-natal origins of childhood leukemia. Rev Clin Exp Hematol. (2003) 7:233–45. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials