

Sarcomatoid carcinoma of the pancreas - multimodality imaging findings with serial imaging follow-up: A case report and review of literature
- PMID: 33969097
- PMCID: PMC8080743
- DOI: 10.12998/wjcc.v9.i13.3102
Sarcomatoid carcinoma of the pancreas - multimodality imaging findings with serial imaging follow-up: A case report and review of literature
Abstract
Background: Sarcomatoid carcinoma of the pancreas is extremely rare and has an extremely poor prognosis. Although a few cases of sarcomatoid carcinoma of pancreas have been reported, most are focused on a histopathological review. To the best of our knowledge, there are no reports documenting multimodality imaging characteristics and chronological changes with emphasis on radiologic features.
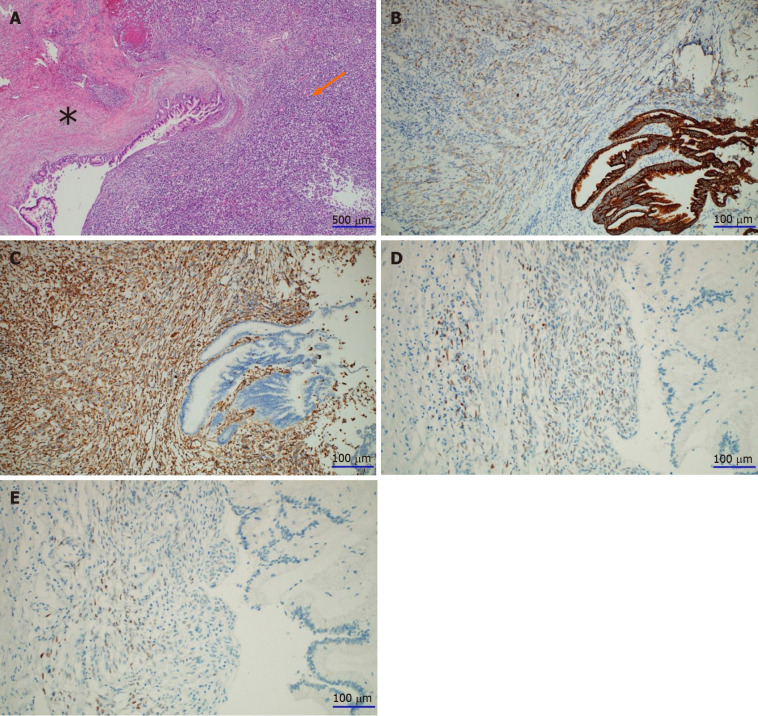
Case summary: A 64-year-old woman was admitted to Chungnam National University Hospital with acute appendicitis. Contrast-enhanced computed tomography of the abdomen revealed a 2.6 cm × 2.8 cm multilobular cystic mass in the pancreatic tail. The pancreatic lesion showed suspected mural nodules and thin septa. Hence, mucinous cystic neoplasm of pancreas was considered. After 7 mo, the patient was readmitted for repeated epigastric abdominal pain and nausea. Follow-up contrast-enhanced computed tomography of the abdomen and magnetic resonance imaging revealed a marked enlargement (5.4 cm × 4 cm), with a predominant internal solid component. The mass showed low signal intensity on a T1-weighted image and heterogeneously intermediate high signal intensity on a T2-weighted image. It showed diffusion restriction and peripheral rim enhancement on an arterial phase image, and progressive enhancement on portal venous and delayed phase images. Distal pancreatectomy was performed. Based on the morphology and immunohistochemical staining of the specimen, pancreatic sarcomatoid carcinoma was diagnosed.
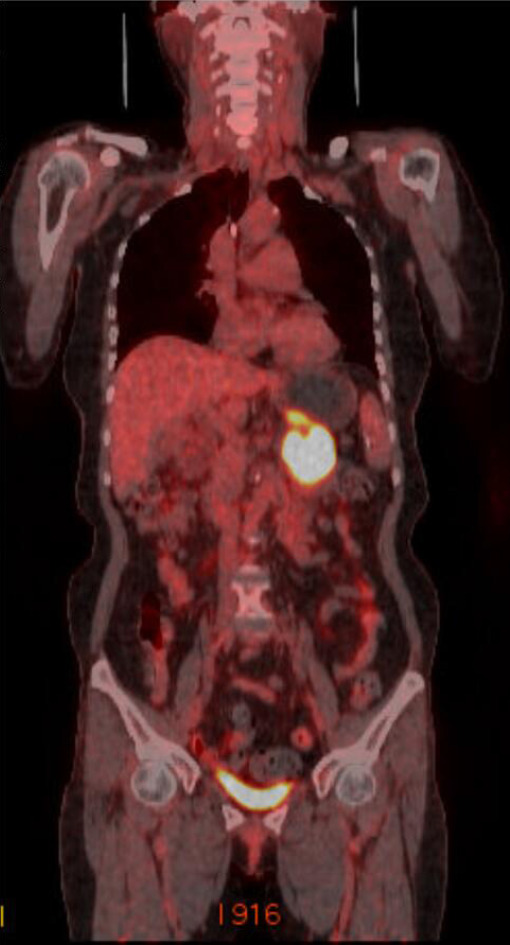
Conclusion: We present the computed tomography, magnetic resonance imaging, and positron emission tomography computed tomography findings, pathologic features, and chronological changes for preoperative diagnosis.
Keywords: Carcinosarcoma; Case report; Computed tomography; Magnetic resonance imaging; Pancreas; Pancreatectomy.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no conflict of interest.
Figures




References
-
- Li J, Wei T, Zhang J, Wei S, Chen Q, Chen BW, Zhou Y, Wen L, Qin H, Bai X, Liang T. Carcinosarcoma of the pancreas: comprehensive clinicopathological and molecular characterization. HPB (Oxford) 2020;22:1590–1595. - PubMed
-
- World Health Organization. WHO classification of tumours: digestive system tumors. 5th ed. Genève, Switzerland: World Health Organization, 2019: 328-329.
-
- Van JD, Snoeks T. Carcinosarcoma of the body of the pancreas. Acta Gastro-enterologica Belgica. 1951;14:106–113. - PubMed
-
- Alhatem A, Quinn PL, Xia W, Chokshi RJ. Pancreatic Carcinosarcoma Clinical Outcome Analysis of the National Cancer Institute Database. J Surg Res. 2021;259:62–70. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
