

Perioperative massive cerebral stroke in thoracic patients: Report of three cases
- PMID: 33969105
- PMCID: PMC8080756
- DOI: 10.12998/wjcc.v9.i13.3170
Perioperative massive cerebral stroke in thoracic patients: Report of three cases
Abstract
Background: Perioperative stroke is a rare but devastating complication. The risk factors for massive cerebral stroke in surgical patients include older age, male sex, prior cerebrovascular disease, hypertension, renal failure, smoking, diabetes mellitus, and atrial fibrillation.
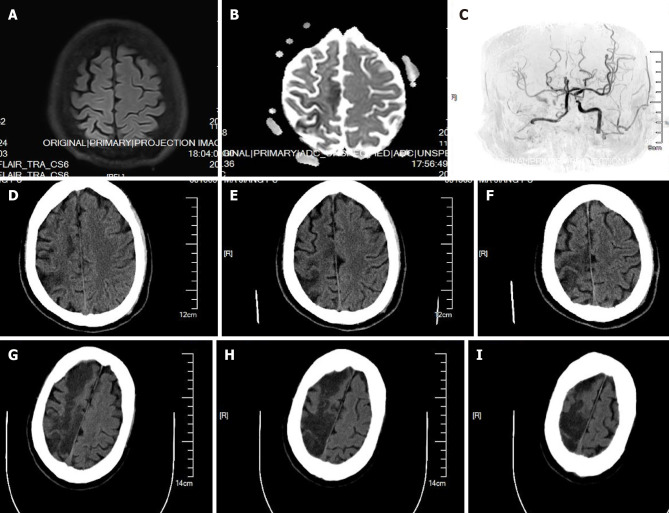
Case summary: We describe two cases of perioperative massive cerebral stroke following thoracic surgery and one case following bronchoscopy. Neurologic symptoms, including changes in mental status and hemiplegia, occurred within 10 h after surgery in the three patients. All three patients died after the surgery.
Conclusion: Perioperative massive cerebral stroke may be more likely to occur in thoracic surgical patients if there are pre-existing factors including previous stroke, hypotension, and hypoxemia. Sufficient pain control after surgery and timely neurology consultation and management are helpful for the diagnosis and control of stroke in high-risk patients.
Keywords: Anesthesia; Case report; Literature review; Massive cerebral stroke; Perioperative; Thoracic surgery.
©The Author(s) 2021. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflict of interest to state.
Figures
Similar articles
-
[Etiologic mechanism and prevention of perioperative stroke].No Shinkei Geka. 2008 May;36(5):409-16. No Shinkei Geka. 2008. PMID: 18516858 Japanese.
-
A retrospective analysis of 62,571 cases of perioperative adverse events in thoracic surgery at a tertiary care teaching hospital in a developing country.J Cardiothorac Surg. 2019 May 31;14(1):98. doi: 10.1186/s13019-019-0921-z. J Cardiothorac Surg. 2019. PMID: 31151461 Free PMC article.
-
Causes of the increased stroke rate after carotid endarterectomy in patients with previous strokes.Ann Vasc Surg. 1997 Jan;11(1):28-34. doi: 10.1007/s100169900006. Ann Vasc Surg. 1997. PMID: 9061136
-
Carotid Artery-Related Perioperative Stroke Following Anterior Cervical Spine Surgery: A Series of 3 Cases and Literature Review.J Stroke Cerebrovasc Dis. 2019 Feb;28(2):458-463. doi: 10.1016/j.jstrokecerebrovasdis.2018.10.024. Epub 2018 Nov 7. J Stroke Cerebrovasc Dis. 2019. PMID: 30413291 Review.
-
Review article: the role of hypotension in perioperative stroke.Can J Anaesth. 2013 Feb;60(2):159-67. doi: 10.1007/s12630-012-9857-7. Epub 2012 Dec 13. Can J Anaesth. 2013. PMID: 23239486 Review.
Cited by
-
Risk factor analysis of postoperative cerebral infarction in thoracic surgery patients by propensity-score matching-a single institution retrospective cohort study.J Thorac Dis. 2023 Feb 28;15(2):620-626. doi: 10.21037/jtd-22-1832. Epub 2023 Feb 23. J Thorac Dis. 2023. PMID: 36910074 Free PMC article.
References
-
- Wong GY, Warner DO, Schroeder DR, Offord KP, Warner MA, Maxson PM, Whisnant JP. Risk of surgery and anesthesia for ischemic stroke. Anesthesiology. 2000;92:425–432. - PubMed
-
- Hsieh JK, Dalton JE, Yang D, Farag ES, Sessler DI, Kurz AM. The Association Between Mild Intraoperative Hypotension and Stroke in General Surgery Patients. Anesth Analg. 2016;123:933–939. - PubMed
-
- Bateman BT, Schumacher HC, Wang S, Shaefi S, Berman MF. Perioperative acute ischemic stroke in noncardiac and nonvascular surgery: incidence, risk factors, and outcomes. Anesthesiology. 2009;110:231–238. - PubMed
-
- Mashour GA, Shanks AM, Kheterpal S. Perioperative stroke and associated mortality after noncardiac, nonneurologic surgery. Anesthesiology. 2011;114:1289–1296. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
