

A urinary peptidomic profile predicts outcome in SARS-CoV-2-infected patients
- PMID: 33969282
- PMCID: PMC8092440
- DOI: 10.1016/j.eclinm.2021.100883
A urinary peptidomic profile predicts outcome in SARS-CoV-2-infected patients
Abstract
Background: COVID-19 prediction models based on clinical characteristics, routine biochemistry and imaging, have been developed, but little is known on proteomic markers reflecting the molecular pathophysiology of disease progression.
Methods: The multicentre (six European study sites) Prospective Validation of a Proteomic Urine Test for Early and Accurate Prognosis of Critical Course Complications in Patients with SARS-CoV-2 Infection Study (Crit-COV-U) is recruiting consecutive patients (≥ 18 years) with PCR-confirmed SARS-CoV-2 infection. A urinary proteomic biomarker (COV50) developed by capillary-electrophoresis-mass spectrometry (CE-MS) technology, comprising 50 sequenced peptides and identifying the parental proteins, was evaluated in 228 patients (derivation cohort) with replication in 99 patients (validation cohort). Death and progression along the World Health Organization (WHO) Clinical Progression Scale were assessed up to 21 days after the initial PCR test. Statistical methods included logistic regression, receiver operating curve (ROC) analysis and comparison of the area under the curve (AUC).
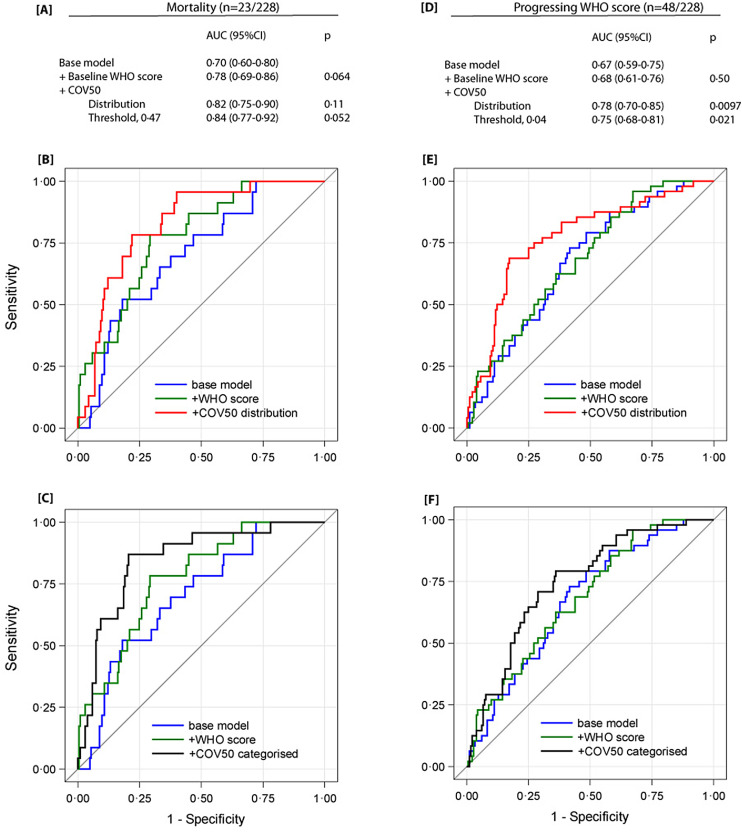
Findings: In the derivation cohort, 23 patients died, and 48 developed worse WHO scores. The odds ratios (OR) for death per 1 standard deviation (SD) increment in COV50 were 3·52 (95% CI, 2·02-6·13, p <0·0001) unadjusted and 2·73 (1·25-5·95, p = 0·012) adjusted for sex, age, baseline WHO score, body mass index (BMI) and comorbidities. For WHO scale progression, the corresponding OR were 2·63 (1·80-3·85, p<0·0001) and 3·38 (1·85-6·17, p<0·0001), respectively. The area under the curve (AUC) for COV50 as a continuously distributed variable was 0·80 (0·72-0·88) for mortality and 0·74 (0·66-0·81) for worsening WHO score. The optimised COV50 thresholds for mortality and worsening WHO score were 0·47 and 0·04 with sensitivity/specificity of 87·0 (74·6%) and 77·1 (63·9%), respectively. On top of covariates, COV50 improved the AUC, albeit borderline for death, from 0·78 to 0·82 (p = 0·11) and 0·84 (p = 0·052) for mortality and from 0·68 to 0·78 (p = 0·0097) and 0·75 (p = 0·021) for worsening WHO score. The validation cohort findings were confirmatory.
Interpretation: This first CRIT-COV-U report proves the concept that urinary proteomic profiling generates biomarkers indicating adverse COVID-19 outcomes, even at an early disease stage, including WHO stages 1-3. These findings need to be consolidated in an upcoming final dataset.
Funding: The German Federal Ministry of Health funded the study.
Keywords: COVID-19; Disease severity; Risk score; SARS-CoV-2; Urinary proteomics.
© 2021 The Author(s).
Conflict of interest statement
AW, BC, BN, HvdL, AN, JB, AM, MM, ACT, BP, KR, CL, RW, SK, ED, JS report payment for study inclusion from the Federal Ministry of Health (Germany) during the conduct of the study; MS reports Scientific Research Activity from Robert Bosch Stiftung during the conduct of the study, grants for clinical trials from Green Cross Wellbeing Co. Ltd. And Gilead Sciences Inc. and grants for research activity from Robert Bosch GmbH, consulting fees as reviewer for Research Impact Fund Hongkong and EU Horizon 2020, honoraria for lectures from CED Service GmbH and ALL Akademie, supporting for meetings from CED Service GmbH and ALL Akademie, participation on advisory board (European PGx Advisory Board) from Agena Bioscience GmbH and other financial interests (Editor) for Phrmacogenetics and Genomics, Drug Research and Genome Medicine; JM, JS and JR are past (JM) or current employees of Mosaiques-Diagnostics, Hanover, Germany, HM is a co-funder and co-owner of Mosaiques-Diagnostics.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
