

Imaging Features of Primary Immunodeficiency Disorders
- PMID: 33969305
- PMCID: PMC8098094
- DOI: 10.1148/ryct.2021200418
Imaging Features of Primary Immunodeficiency Disorders
Abstract
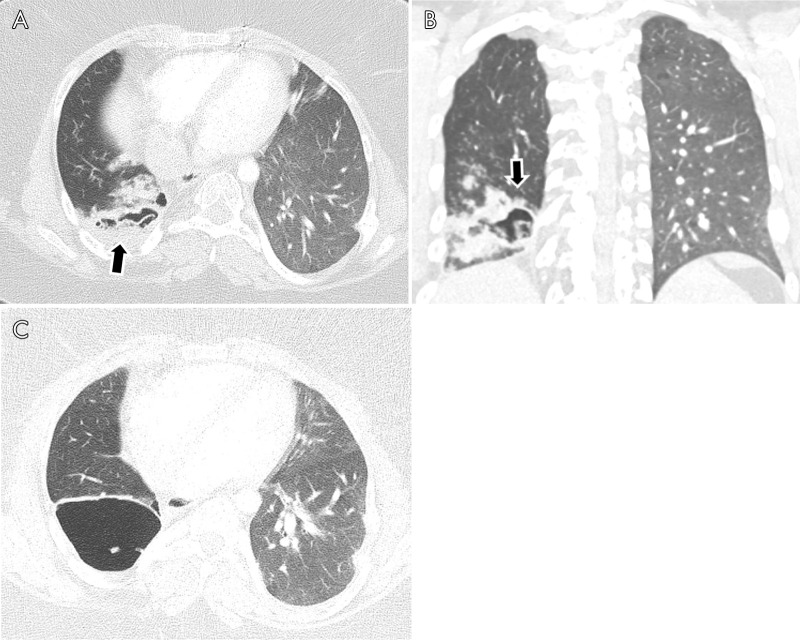
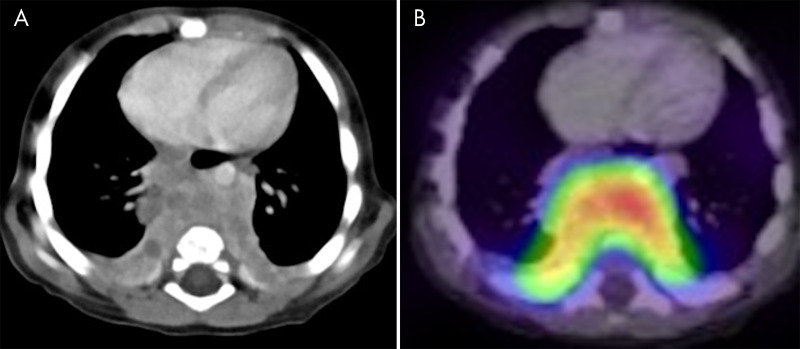
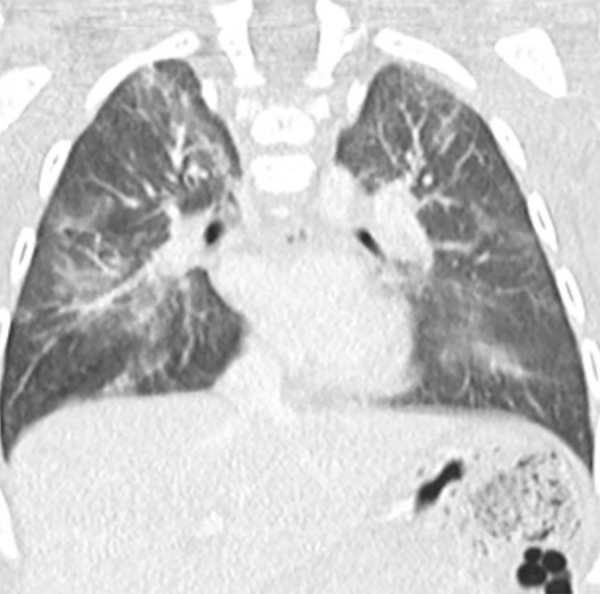
Primary immunodeficiency disorders (PIDs), which are humoral, combined, and innate defects of the immune system, are relatively uncommon and may go undiagnosed in patients experiencing recurrent infections, resulting in increased morbidity and mortality. PIDs are clinically characterized by a broad spectrum of disorders, including repeated infections, autoimmune disorders, lymphoproliferative diseases, congenital anomalies, and increased risk of malignancy. Cardiothoracic imaging plays a crucial role in the diagnosis of PIDs owing to the high rates of repeated respiratory infections leading to bronchiectasis and other forms of chronic lung disease. Although PIDs as a group may seem similar in terms of radiologic features and clinical manifestations, there are specific entities that are pertinent to each PID on an individual level. For example, patients with common variable immunodeficiency may develop a unique granulomatous lymphocytic interstitial lung disease, and Good syndrome is associated with thymoma. Familiarity with the imaging characteristics of these disorders may expedite diagnosis and prognostication, and better direct therapy. Reviewing the thoracic manifestations of all PIDs is beyond the scope of this article; thus, the focus herein is on discussing the thoracic manifestations of the most common PIDs and their imaging features. © RSNA, 2021An earlier incorrect version appeared online. This article was corrected on March 25, 2021.
2021 by the Radiological Society of North America, Inc.
Conflict of interest statement
Disclosures of Conflicts of Interest: J.A.R. disclosed no relevant relationships. T.J.B. disclosed no relevant relationships. C.S.R. disclosed no relevant relationships. D.B.G. disclosed no relevant relationships. L.P.B. disclosed no relevant relationships. D.V. disclosed no relevant relationships.
Figures










References
-
- Booth C, Romano R, Roncarolo MG, Thrasher AJ. Gene therapy for primary immunodeficiency. Hum Mol Genet 2019;28(R1):R15–R23. - PubMed
-
- D’Angelo P, Cereser L, Bednarova S, Carli MD, Pellegrin AD, Zuiani C. Chest HRCT findings in patients with humoral Primary Immunodeficiencies and recurrent respiratory infections: review of literature and personal experience. European Society of Radiology, 2017.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
