

Lung Ultrasound: The Essentials
- PMID: 33969313
- PMCID: PMC8098095
- DOI: 10.1148/ryct.2021200564
Lung Ultrasound: The Essentials
Abstract
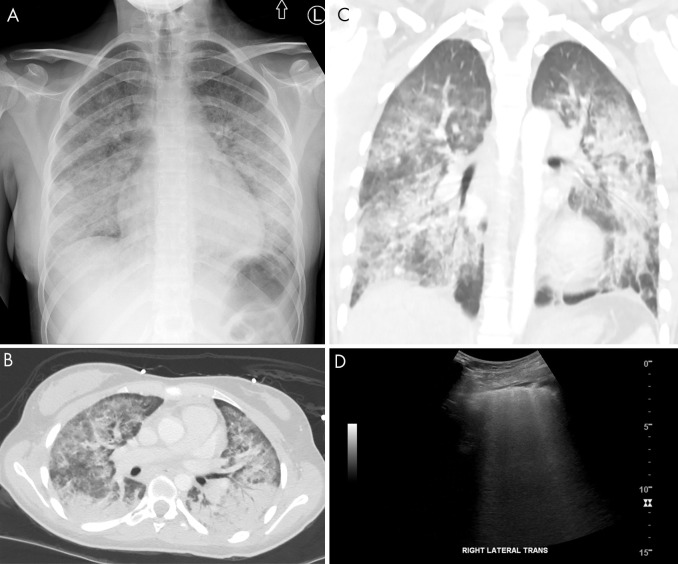
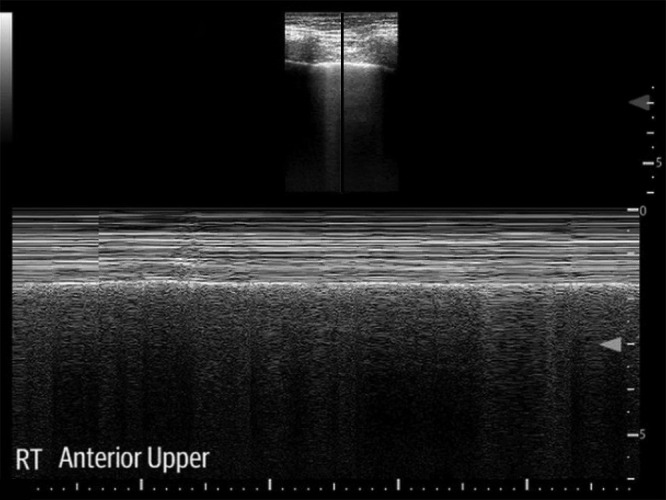
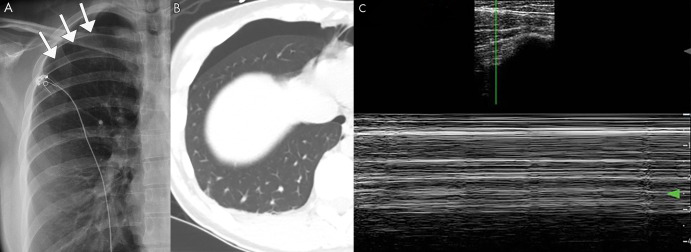
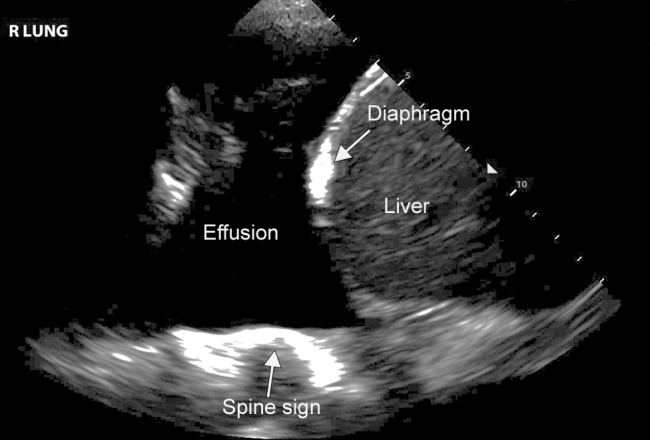
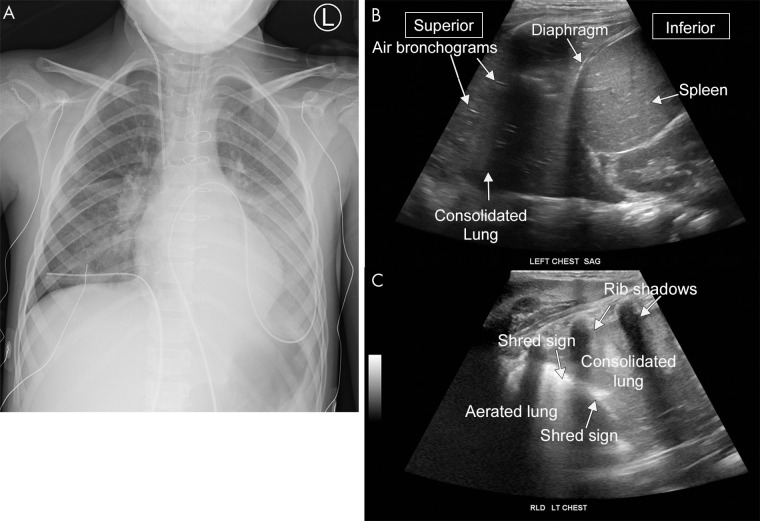
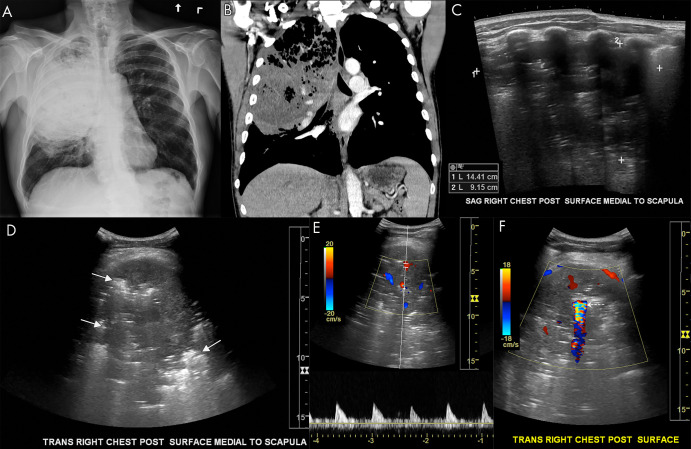
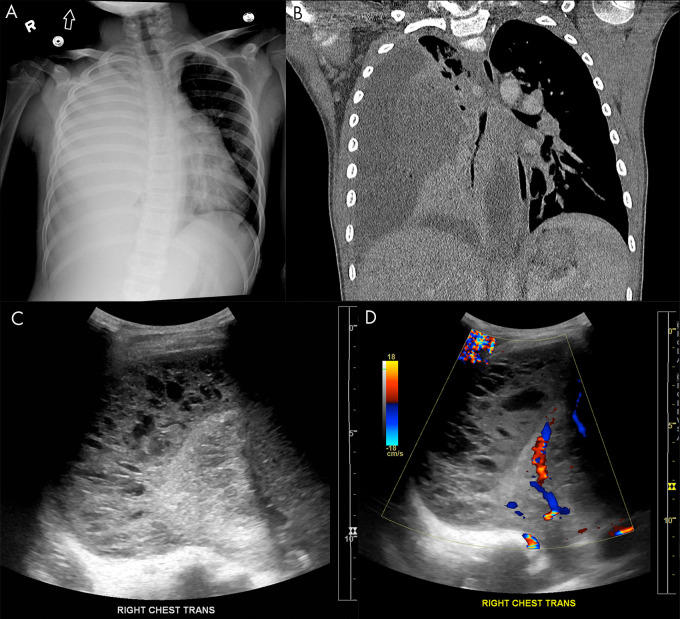
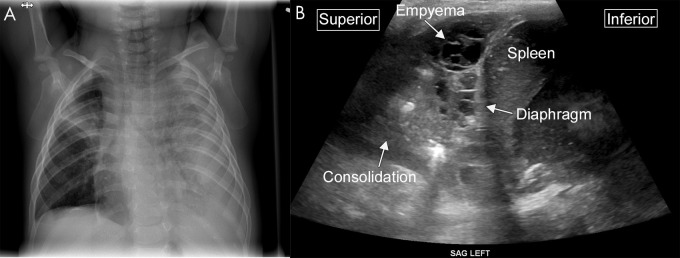
Although US of the lungs is increasingly used clinically, diagnostic radiologists are not routinely trained in its use and interpretation. Lung US is a highly sensitive and specific modality that aids in the evaluation of the lungs for many different abnormalities, including pneumonia, pleural effusion, pulmonary edema, and pneumothorax. This review provides an overview of lung US to equip the diagnostic radiologist with knowledge needed to interpret this increasingly used modality. Supplemental material is available for this article. © RSNA, 2021.
2021 by the Radiological Society of North America, Inc.
Conflict of interest statement
Disclosures of Conflicts of Interest: T.J.M. disclosed no relevant relationships. D.J.R. disclosed no relevant relationships. Y.T.Z. disclosed no relevant relationships. J.W. disclosed no relevant relationships. T.P.O. disclosed no relevant relationships. W.H.N. disclosed no relevant relationships. K.A.K.J. disclosed no relevant relationships.
Figures

References
-
- Lichtenstein DA. Current Misconceptions in Lung Ultrasound: A Short Guide for Experts. Chest 2019;156(1):21–25. - PubMed
-
- Lichtenstein D, Goldstein I, Mourgeon E, Cluzel P, Grenier P, Rouby JJ. Comparative diagnostic performances of auscultation, chest radiography, and lung ultrasonography in acute respiratory distress syndrome. Anesthesiology 2004;100(1):9–15. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
