

Longitudinal proteomic analysis of severe COVID-19 reveals survival-associated signatures, tissue-specific cell death, and cell-cell interactions
- PMID: 33969320
- PMCID: PMC8091031
- DOI: 10.1016/j.xcrm.2021.100287
Longitudinal proteomic analysis of severe COVID-19 reveals survival-associated signatures, tissue-specific cell death, and cell-cell interactions
Abstract
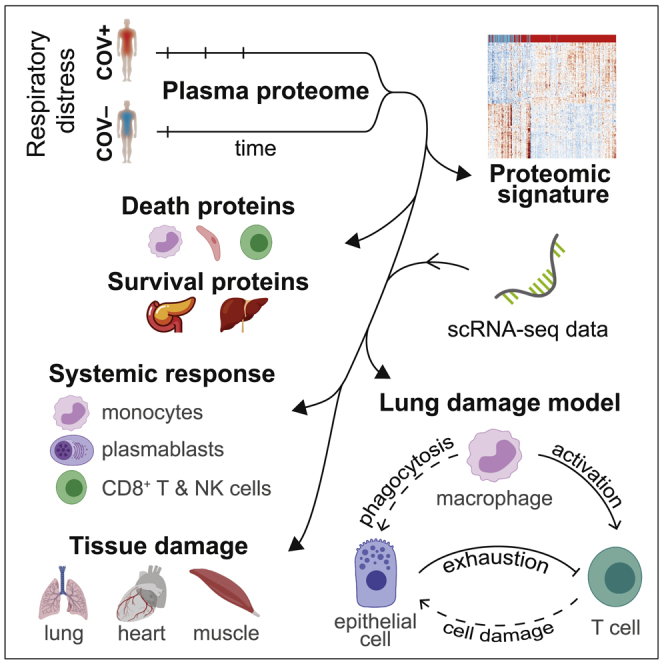
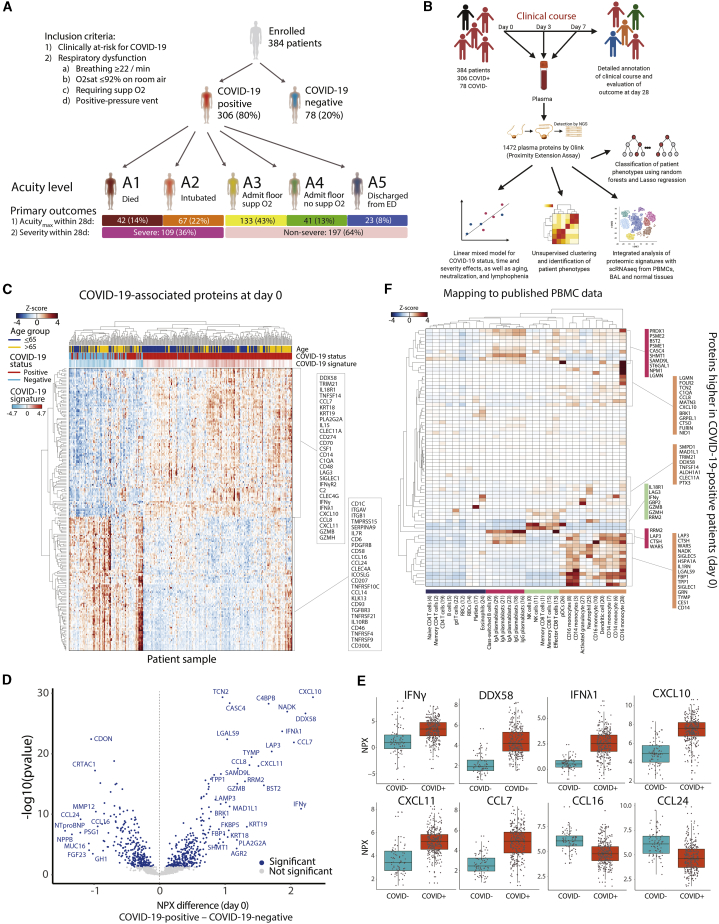
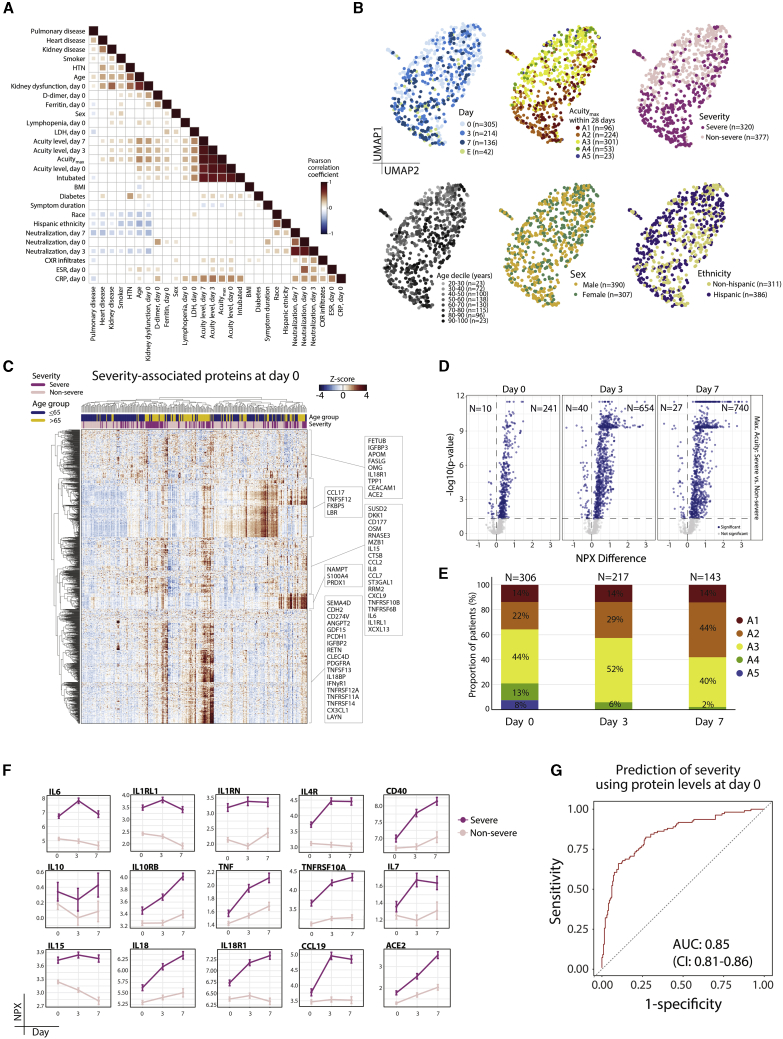
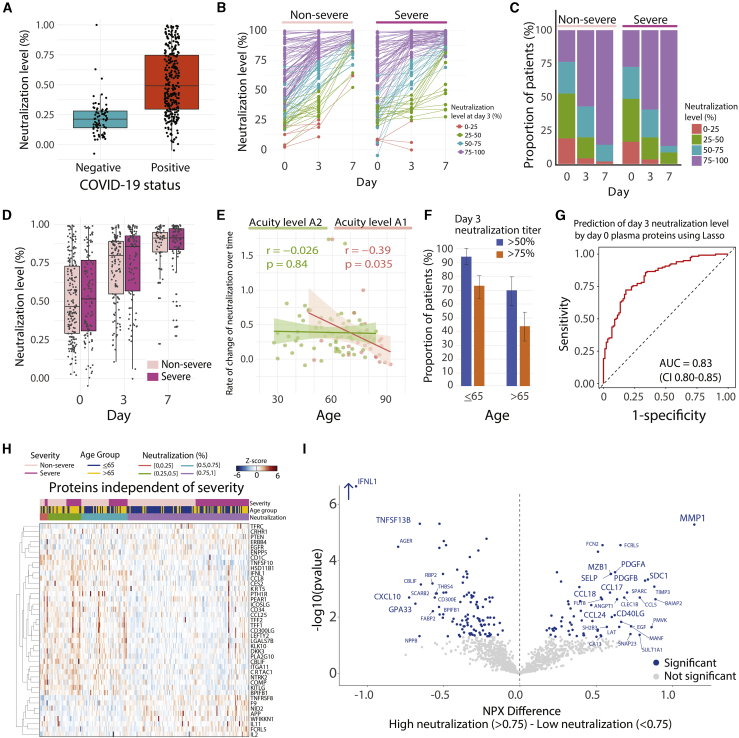
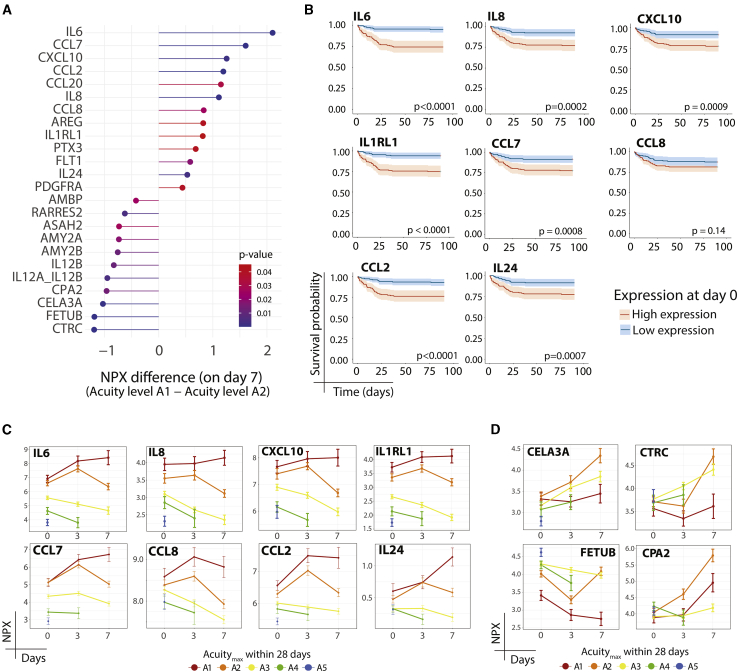
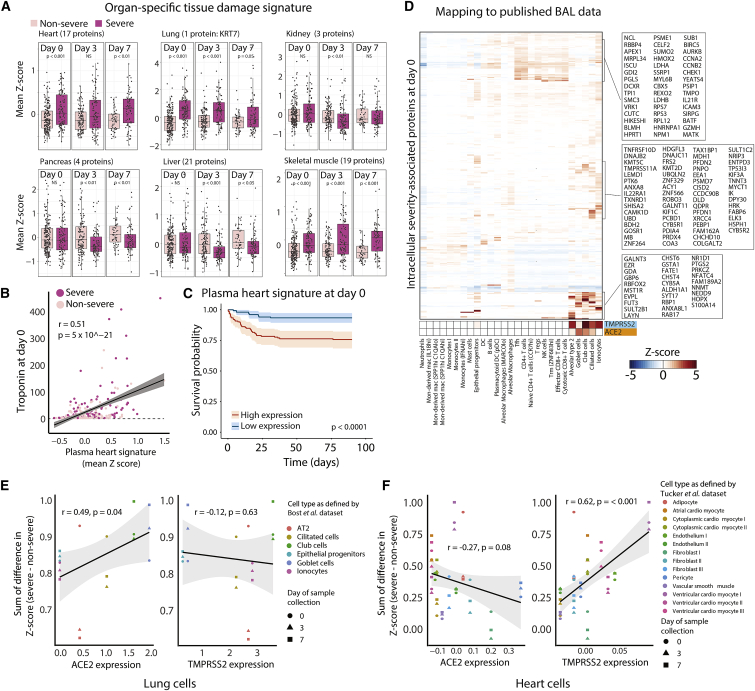
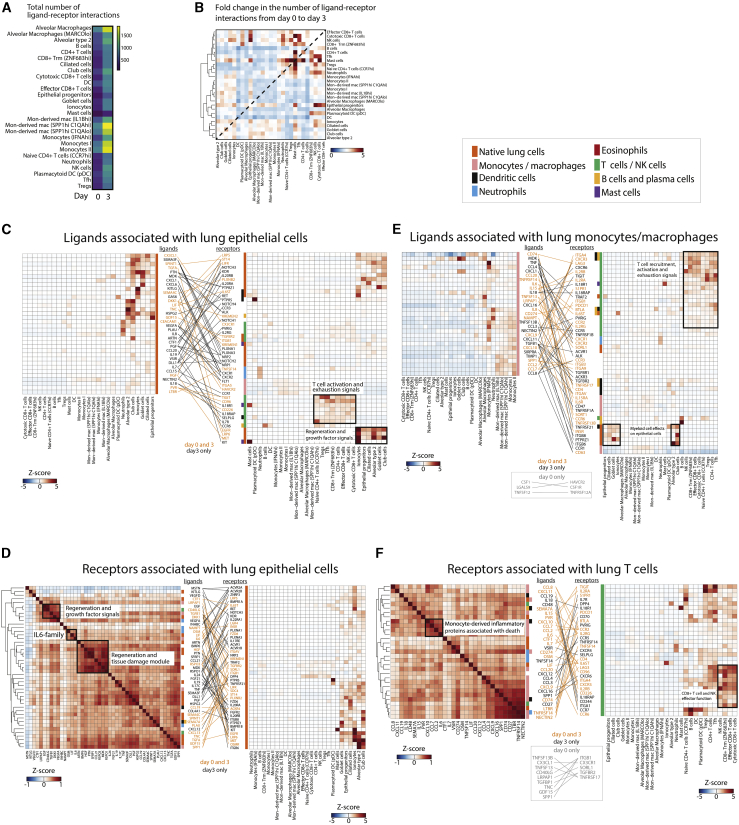
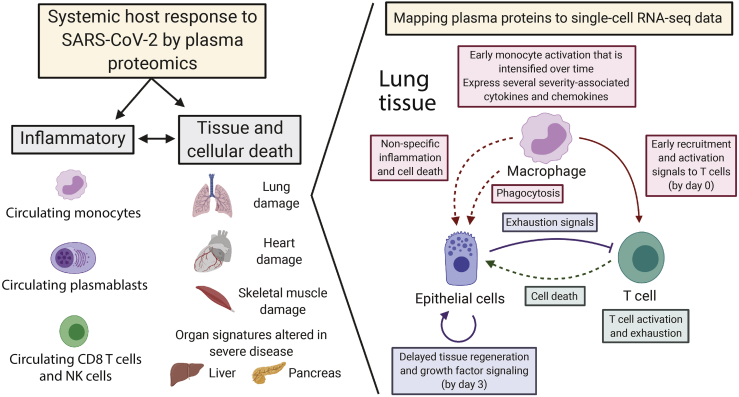
Mechanisms underlying severe coronavirus disease 2019 (COVID-19) disease remain poorly understood. We analyze several thousand plasma proteins longitudinally in 306 COVID-19 patients and 78 symptomatic controls, uncovering immune and non-immune proteins linked to COVID-19. Deconvolution of our plasma proteome data using published scRNA-seq datasets reveals contributions from circulating immune and tissue cells. Sixteen percent of patients display reduced inflammation yet comparably poor outcomes. Comparison of patients who died to severely ill survivors identifies dynamic immune-cell-derived and tissue-associated proteins associated with survival, including exocrine pancreatic proteases. Using derived tissue-specific and cell-type-specific intracellular death signatures, cellular angiotensin-converting enzyme 2 (ACE2) expression, and our data, we infer whether organ damage resulted from direct or indirect effects of infection. We propose a model in which interactions among myeloid, epithelial, and T cells drive tissue damage. These datasets provide important insights and a rich resource for analysis of mechanisms of severe COVID-19 disease.
Keywords: ARDS; COVID-19 severity; T cell activation; acute respiratory distress syndrome; death versus survival; intracellular death signatures; longitudinal; lung epithelial cells; lung monocyte/macrophages; pancreatic exocrine proteases; plasma proteomics.
© 2021 The Authors.
Conflict of interest statement
A.M. is a consultant for Third Rock Ventures. J.R.G. and I. Gushterova are employees of Olink Proteomics. G.S.H. is an employee of Genentech (as of November 2020). L.L.J. is an employee and stockholder of Novartis. N.H. holds equity in BioNTech and is a consultant for Related Sciences.
Figures
Update of
-
Plasma proteomics reveals tissue-specific cell death and mediators of cell-cell interactions in severe COVID-19 patients.bioRxiv [Preprint]. 2020 Nov 4:2020.11.02.365536. doi: 10.1101/2020.11.02.365536. bioRxiv. 2020. Update in: Cell Rep Med. 2021 May 18;2(5):100287. doi: 10.1016/j.xcrm.2021.100287. PMID: 33173871 Free PMC article. Updated. Preprint.
References
-
- Mathew D., Giles J.R., Baxter A.E., Oldridge D.A., Greenplate A.R., Wu J.E., Alanio C., Kuri-Cervantes L., Pampena M.B., D’Andrea K., UPenn COVID Processing Unit Deep immune profiling of COVID-19 patients reveals distinct immunotypes with therapeutic implications. Science. 2020;369:eabc8511. - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
