

Changes in COVID-19 in-hospital mortality in hospitalised adults in England over the first seven months of the pandemic: An observational study using administrative data
- PMID: 33969337
- PMCID: PMC8086562
- DOI: 10.1016/j.lanepe.2021.100104
Changes in COVID-19 in-hospital mortality in hospitalised adults in England over the first seven months of the pandemic: An observational study using administrative data
Abstract
Background: Previous research by our team identified factors associated with in-hospital mortality in patients with a diagnosis of COVID-19 in England between March and May 2020. The aim of the current paper was to investigate the changing role of demographics and co-morbidity, with a particular focus on ethnicity, as risk factors for in-hospital mortality over an extended period.
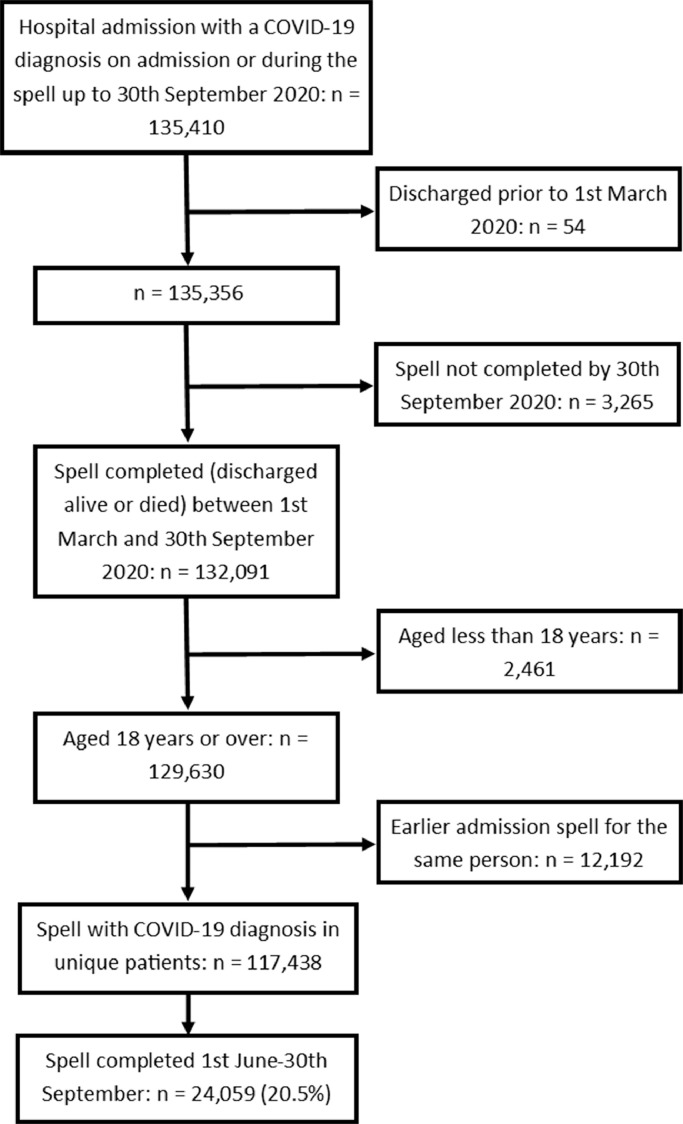
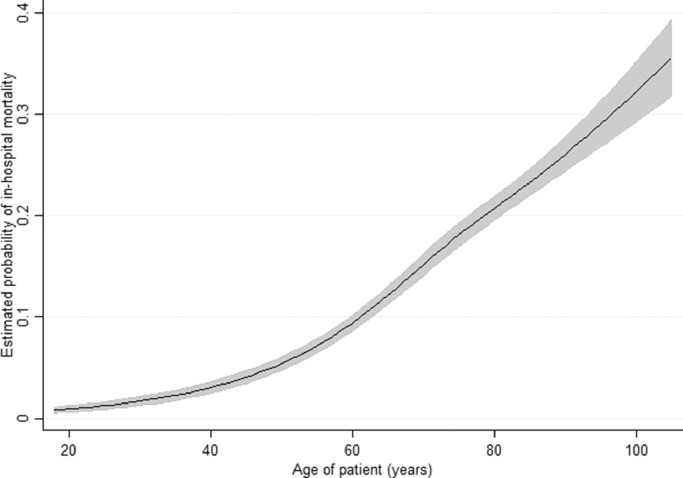
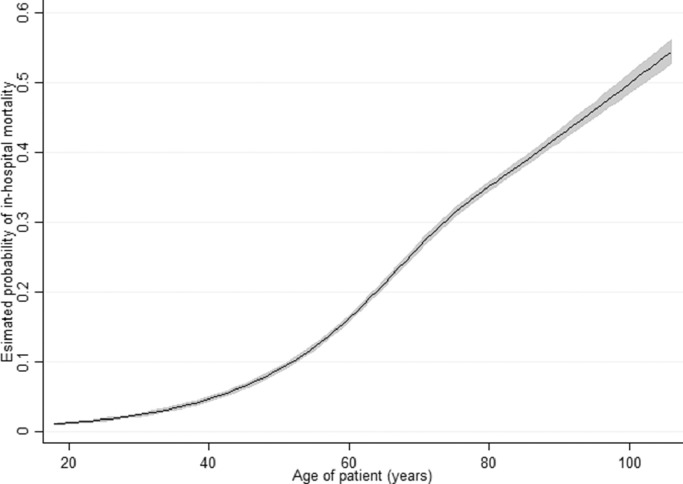
Methods: This was a retrospective observational study using the Hospital Episode Statistics administrative dataset. All patients aged ≥ 18 years in England with a diagnosis of COVID-19 who had a hospital stay that was completed (discharged alive or died) between 1st March and 30th September 2020 were included. In-hospital mortality was the primary outcome of interest. Multilevel logistic regression was used to model the relationship between in-hospital mortality with adjustment for the covariates: age, sex, deprivation, ethnicity, date of discharge and a number of comorbidities.
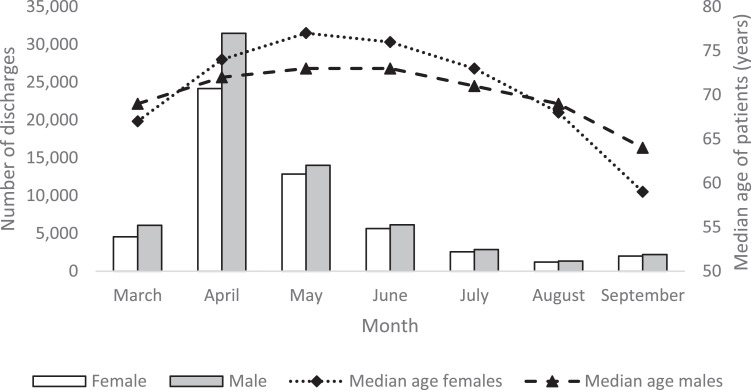
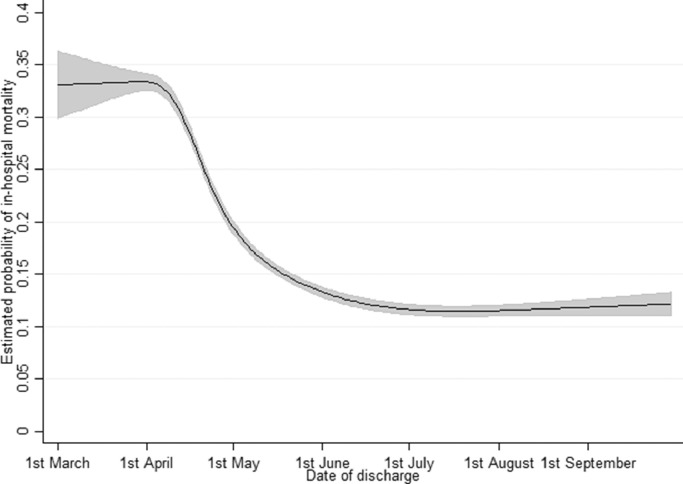
Findings: Compared to patients in March-May (n = 93,379), patients in June-September (n = 24,059) were younger, more likely to be female and of Asian ethnicity, but less likely to be of Black ethnicity. In-hospital mortality rates, adjusted for covariates, declined from 33-34% in March to 11-12% in September. Compared to the March-May period, Bangladeshi, Indian and Other Asian ethnicity patients had a lower relative odds of death (compared to White ethnicity patients) during June-September. For Pakistani patients, the decline in-hospital mortality rates was more modest across the same time periods with the relative odds of death increasing slightly (odds ratio (95% confidence interval)) 1.24 (1.10 to 1.40) and 1.35 (1.08 to 1.69) respectively. From March-May to June-September the relative odds of death in patients with a diagnosis of metastatic carcinoma increased (1.90 (1.73 to 2.08) vs 3.01 (2.55 to 3.54)) but decreased for male patients (1.44 (1.39 to 1.49) vs 1.27 (1.17 to 1.38)) and patients with obesity (1.42 (1.34 to 1.52) vs 0.97 (0.83 to 1.14)) and diabetes without complications (1.14 (1.10 to 1.19) vs 0.95 (0.87 to 1.05)).
Interpretation: In-hospital mortality rates for patients with a diagnosis of COVID-19 have fallen substantially and there is evidence that the relative importance of some covariates has changed since the start of the pandemic. These patterns should continue to be tracked as new variants of the virus emerge, vaccination programmes are rolled out and hospital pressures fluctuate.
Keywords: COVID-19; Coronavirus; Ethnicity; Mortality; Risk factors.
© 2021 The Authors.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Figures
References
-
- Navaratnam A.V., Gray W.K., Day J., Wendon J., Briggs T.W.R. Patient factors and temporal trends associated with COVID-19 in-hospital mortality in England: an observational study using administrative data. Lancet Respir Med. 2021;9(4):397–406. doi: 10.1016/S2213-2600(20)30579-8. Accepted for publication. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
