

RFC1 expansions are a common cause of idiopathic sensory neuropathy
- PMID: 33969391
- PMCID: PMC8262986
- DOI: 10.1093/brain/awab072
RFC1 expansions are a common cause of idiopathic sensory neuropathy
Abstract
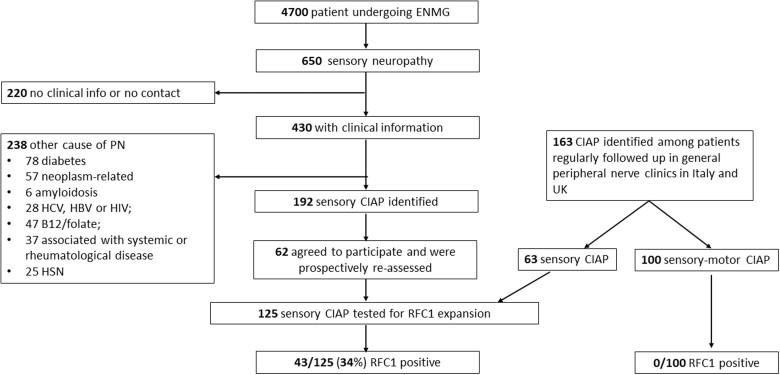
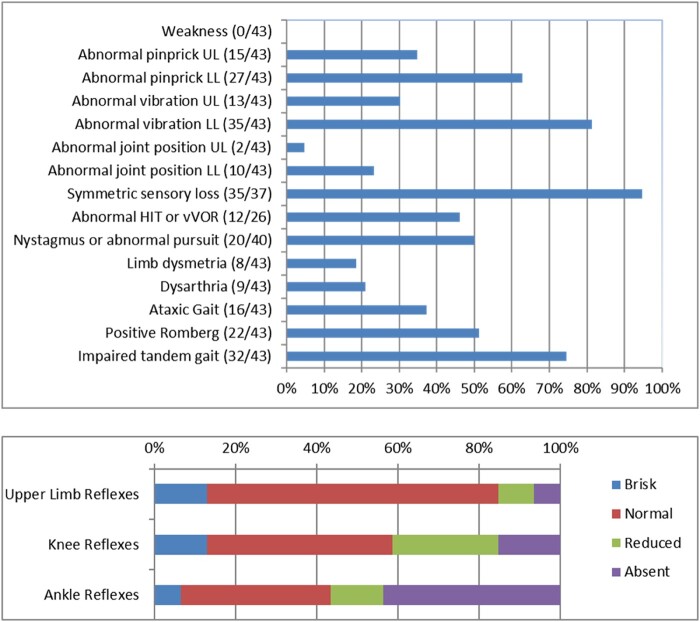
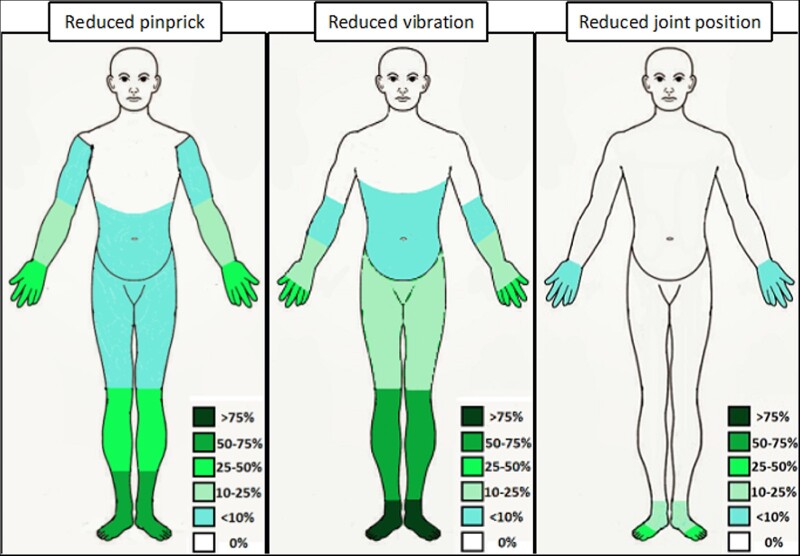
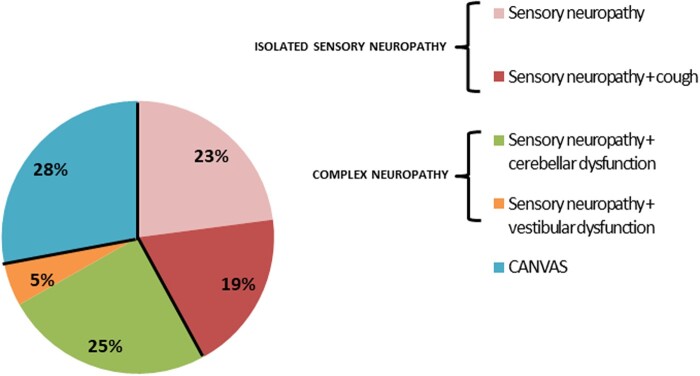
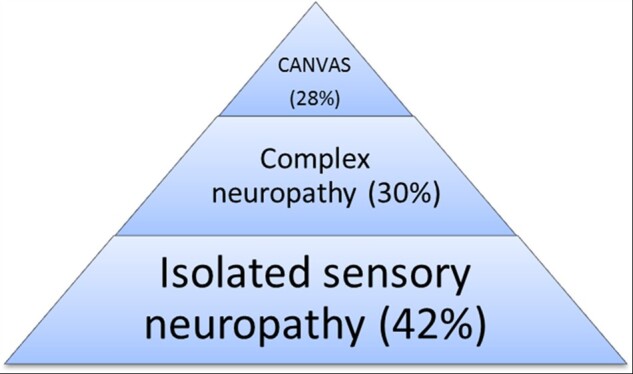
After extensive evaluation, one-third of patients affected by polyneuropathy remain undiagnosed and are labelled as having chronic idiopathic axonal polyneuropathy, which refers to a sensory or sensory-motor, axonal, slowly progressive neuropathy of unknown origin. Since a sensory neuropathy/neuronopathy is identified in all patients with genetically confirmed RFC1 cerebellar ataxia, neuropathy, vestibular areflexia syndrome, we speculated that RFC1 expansions could underlie a fraction of idiopathic sensory neuropathies also diagnosed as chronic idiopathic axonal polyneuropathy. We retrospectively identified 225 patients diagnosed with chronic idiopathic axonal polyneuropathy (125 sensory neuropathy, 100 sensory-motor neuropathy) from our general neuropathy clinics in Italy and the UK. All patients underwent full neurological evaluation and a blood sample was collected for RFC1 testing. Biallelic RFC1 expansions were identified in 43 patients (34%) with sensory neuropathy and in none with sensory-motor neuropathy. Forty-two per cent of RFC1-positive patients had isolated sensory neuropathy or sensory neuropathy with chronic cough, while vestibular and/or cerebellar involvement, often subclinical, were identified at examination in 58%. Although the sensory ganglia are the primary pathological target of the disease, the sensory impairment was typically worse distally and symmetric, while gait and limb ataxia were absent in two-thirds of the cases. Sensory amplitudes were either globally absent (26%) or reduced in a length-dependent (30%) or non-length dependent pattern (44%). A quarter of RFC1-positive patients had previously received an alternative diagnosis, including Sjögren's syndrome, sensory chronic inflammatory demyelinating polyneuropathy and paraneoplastic neuropathy, while three cases had been treated with immune therapies.
Keywords: CANVAS; RFC1; chronic idiopathic axonal polyneuropathy; sensory neuropathy.
© The Author(s) (2021). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
Comment in
-
Removing the idiopathic from the chronic sensory neuropathies.Brain. 2021 Jun 22;144(5):1291-1292. doi: 10.1093/brain/awab150. Brain. 2021. PMID: 33983437 Free PMC article.
-
Sensory axonal neuropathy in RFC1-disease: tip of the iceberg of broad subclinical multisystemic neurodegeneration.Brain. 2022 Apr 29;145(3):e6-e9. doi: 10.1093/brain/awac003. Brain. 2022. PMID: 35230382 No abstract available.
References
-
- Farhad K, Traub R, Ruzhansky KM, Brannagan TH.. Causes of neuropathy in patients referred as “idiopathic neuropathy”. Muscle Nerve. 2016;53:856–861. - PubMed
-
- Pasnoor M, Nascimento OJM, Trivedi J, et al.North America and South America (NA-SA) neuropathy project. Int J Neurosci. 2013;123:563–567. - PubMed
-
- Smith AG, Singleton JR.. The diagnostic yield of a standardized approach to idiopathic sensory-predominant neuropathy. Arch Intern Med. 2004;164:1021–1025. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
