

Recovery of consciousness and cognition after general anesthesia in humans
- PMID: 33970101
- PMCID: PMC8163502
- DOI: 10.7554/eLife.59525
Recovery of consciousness and cognition after general anesthesia in humans
Abstract
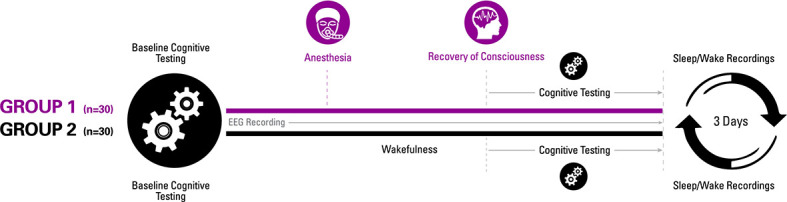
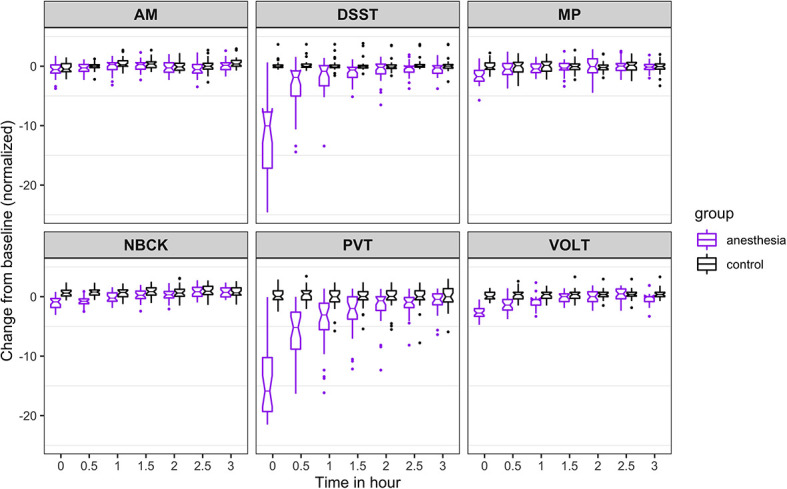
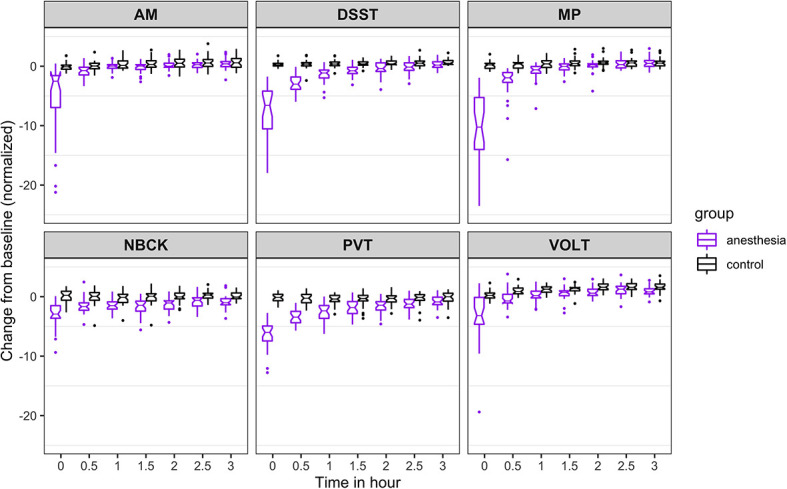
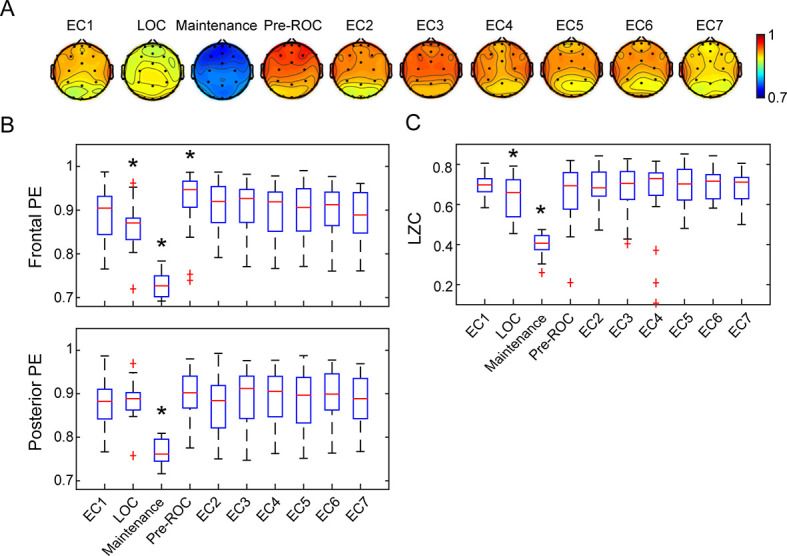
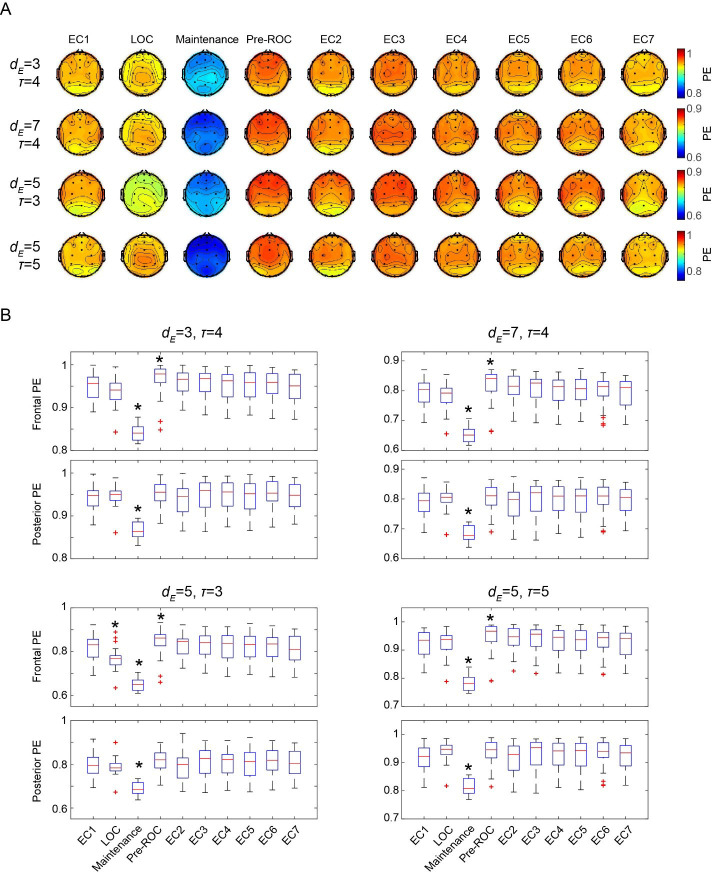
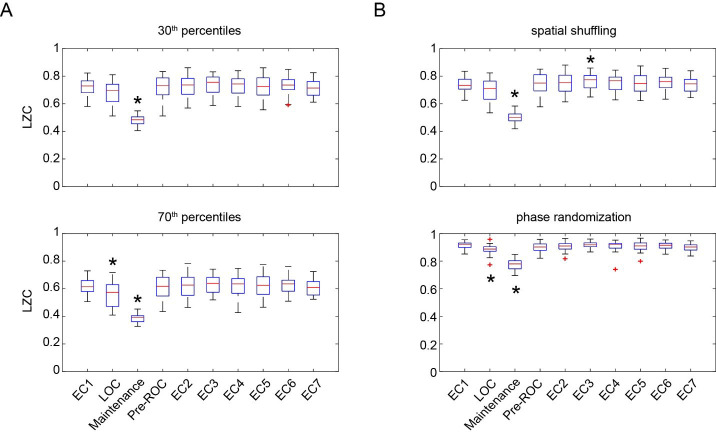
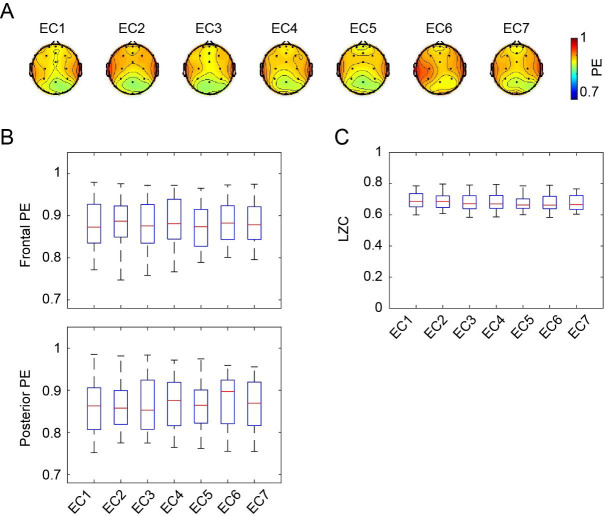
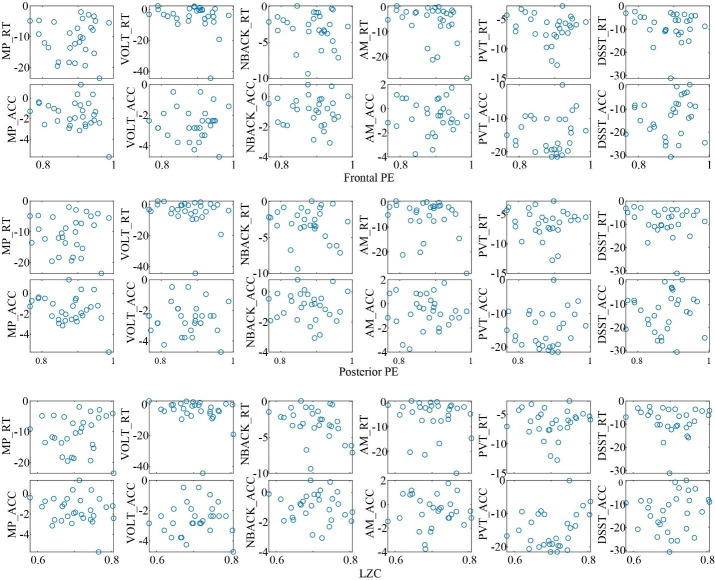
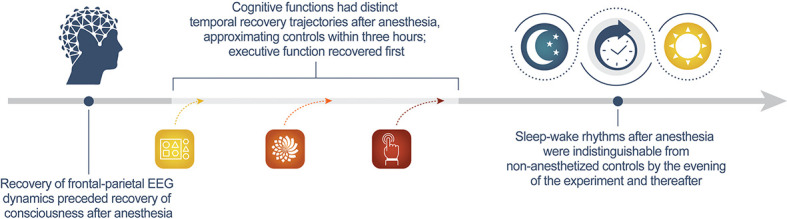
Understanding how the brain recovers from unconsciousness can inform neurobiological theories of consciousness and guide clinical investigation. To address this question, we conducted a multicenter study of 60 healthy humans, half of whom received general anesthesia for 3 hr and half of whom served as awake controls. We administered a battery of neurocognitive tests and recorded electroencephalography to assess cortical dynamics. We hypothesized that recovery of consciousness and cognition is an extended process, with differential recovery of cognitive functions that would commence with return of responsiveness and end with return of executive function, mediated by prefrontal cortex. We found that, just prior to the recovery of consciousness, frontal-parietal dynamics returned to baseline. Consistent with our hypothesis, cognitive reconstitution after anesthesia evolved over time. Contrary to our hypothesis, executive function returned first. Early engagement of prefrontal cortex in recovery of consciousness and cognition is consistent with global neuronal workspace theory.
Trial registration: ClinicalTrials.gov NCT01911195.
Keywords: anesthesia; cognition; consciousness; frontal cortex; human; medicine; neuroscience.
Plain language summary
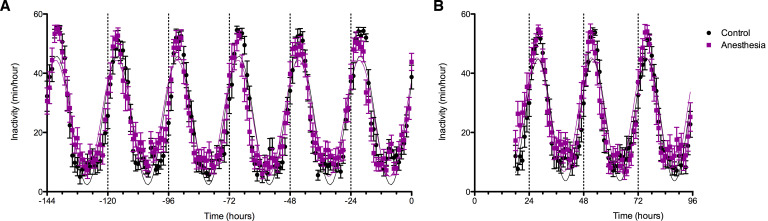
Anesthesia is a state of reversable, controlled unconsciousness. It has enabled countless medical procedures. But it also serves as a tool for scientists to study how the brain regains consciousness after disruptions such as sleep, coma or medical procedures requiring general anesthesia. It is still unclear how exactly the brain regains consciousness, and less so, why some patients do not recover normally after general anesthesia or fail to recover from brain injury. To find out more, Mashour et al. studied the patterns of reemerging consciousness and cognitive function in 30 healthy adults who underwent general anesthesia for three hours. While the volunteers were under anesthesia, their brain activity was measured with an EEG; and their sleep-wake activity was measured before and after the experiment. Each participant took part in a series of cognitive tests designed to measure the reaction speed, memory and other functions before receiving anesthesia, right after the return of consciousness, and then every 30 minutes thereafter. Thirty healthy volunteers who did not have anesthesia also completed the scans and tests as a comparison group. The experiments showed that certain normal EEG patterns resumed just before a person wakes up from anesthesia. The return of thinking abilities was an extended, multistep process, but volunteers recovered their cognitive abilities to nearly the same level as the volunteers within three hours of being deeply anesthetized. Mashour et al. also unexpectedly found that abstract problem-solving resumes early in the process, while other functions such as reaction time and attention took longer to recover. This makes sense from an evolutionary perspective. Sleep leaves individuals vulnerable. Quick evaluation and decision-making skills would be key to respond to a threat upon waking. The experiments confirm that the front of the brain, which handles thinking and decision-making, was especially active around the time of recovery. This suggests that therapies targeting this part of the brain may help people who experience loss of consciousness after a brain injury or have difficulties waking up after anesthesia. Moreover, disorders of cognition, such as delirium, in the days following surgery may be caused by factors other than the lingering effects of anesthetic drugs on the brain.
© 2021, Mashour et al.
Conflict of interest statement
GM, BP, MB, DL, WW, SB, NL, KM, MM, VT, GV, EO, RH, MS, HM, RH, EJ, GG, PP, AM, MA, MK No competing interests declared
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
