

Assessment of Recurrent Stroke Risk in Patients With a Carotid Web
- PMID: 33970205
- PMCID: PMC8111564
- DOI: 10.1001/jamaneurol.2021.1101
Assessment of Recurrent Stroke Risk in Patients With a Carotid Web
Abstract
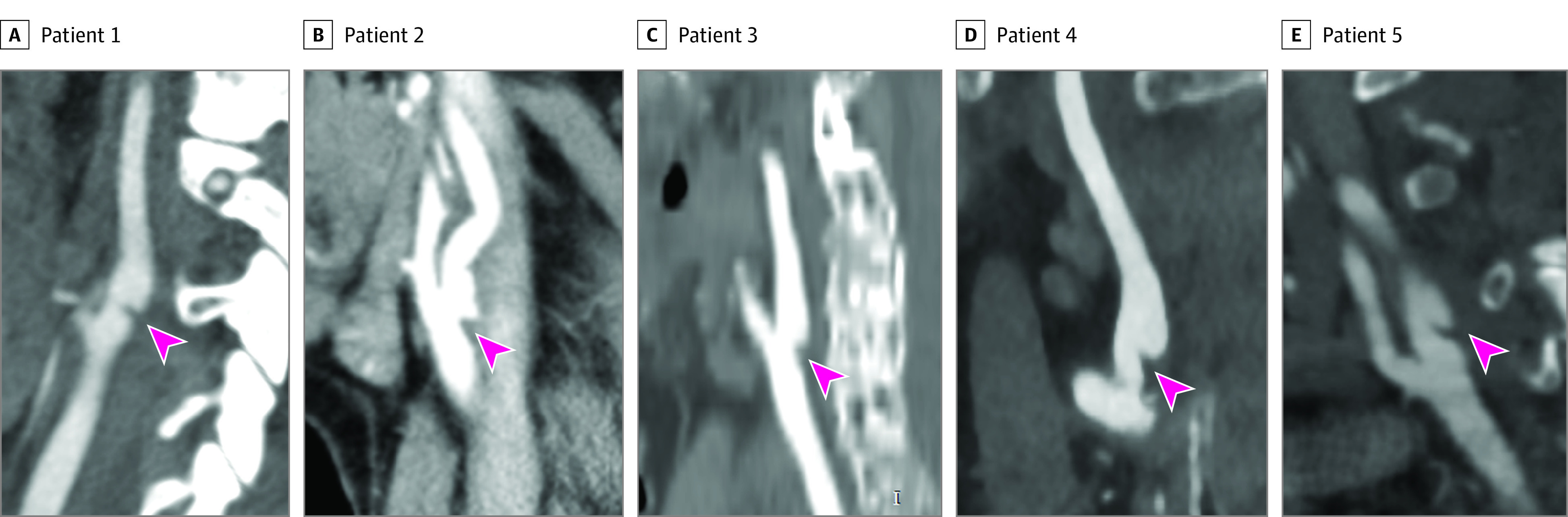
Importance: A carotid web (CW) is a shelf-like lesion along the posterior wall of the internal carotid artery bulb and an underrecognized cause of young stroke. Several studies suggest that patients with symptomatic CW have a high risk of recurrent stroke, but high-quality data are lacking.
Objective: To assess the 2-year risk of recurrent stroke in patients with a symptomatic CW.
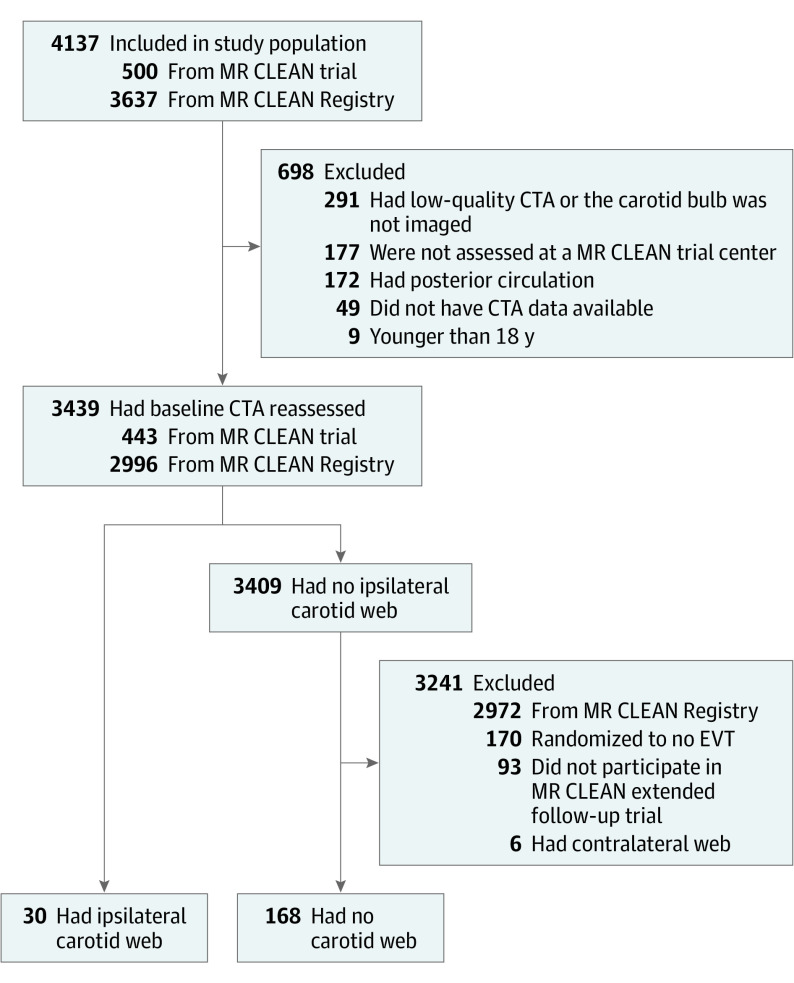
Design, setting, and participants: A comparative cohort study used data from the MR CLEAN trial (from 2010-2014) and MR CLEAN Registry (from 2014-2017). Data were analyzed in September 2020. The MR CLEAN trial and MR CLEAN Registry were nationwide prospective multicenter studies on endovascular treatment (EVT) of large vessel occlusion (LVO) stroke in the Netherlands. Baseline data were from 3439 consecutive adult patients with anterior circulation LVO stroke and available computed tomography (CT)-angiography of the carotid bulb. Two neuroradiologists reevaluated CT-angiography images for presence or absence of CW and identified 30 patients with CW ipsilateral to the index stroke. For these 30 eligible CW participants, detailed follow-up data regarding stroke recurrence within 2 years were acquired. These 30 patients with CW ipsilateral to the index stroke were compared with 168 patients without CW who participated in the MR CLEAN extended follow-up trial and who were randomized to the EVT arm.
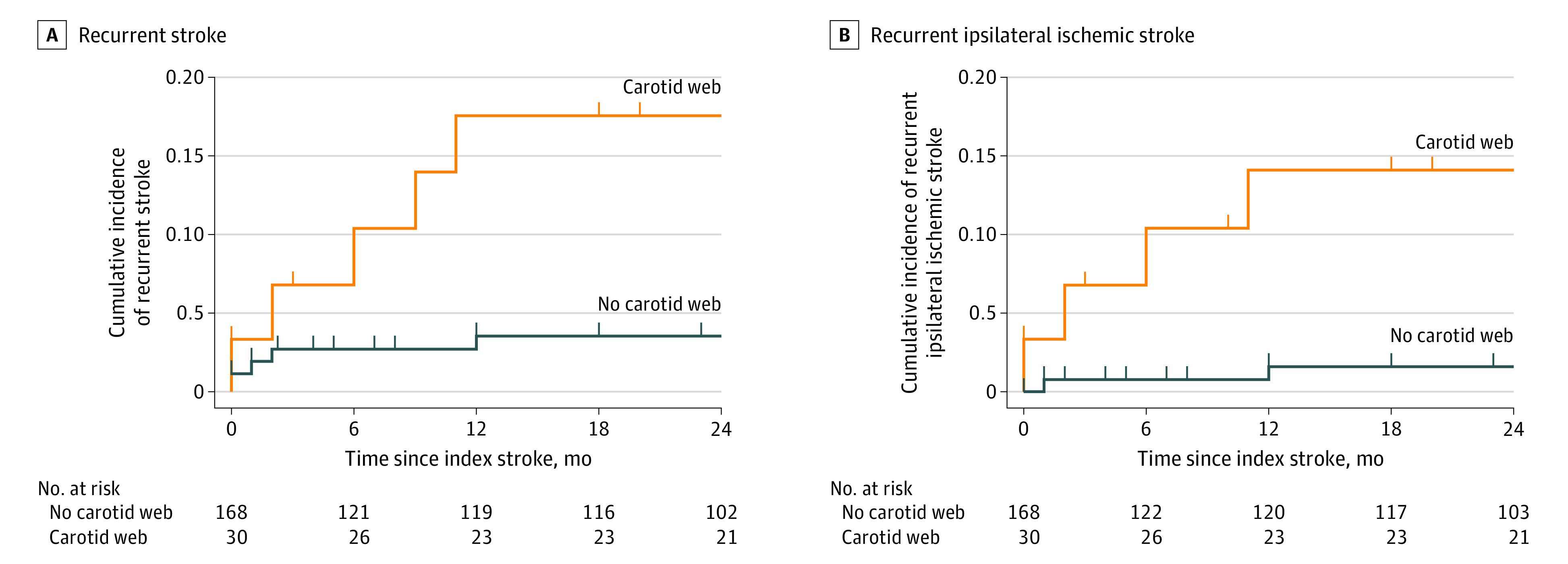
Main outcomes and measures: The primary outcome was recurrent stroke occurring within 2 years after the index stroke. Cox proportional hazards regression models were used to compare recurrent stroke rates within 2 years for patients with and without CW, adjusted for age and sex. The research question was formulated prior to data collection.
Results: Of 3439 patients with baseline CT-angiography assessed, the median age was 72 years (interquartile range, 61-80 years) and 1813 (53%) were men. Patients with CW were younger (median age, 57 [interquartile range, 46-66] years vs 66 [interquartile range, 56-77] years; P = .02 and more often women (22 of 30 [73%] vs 67 of 168 [40%]; P = .001) than patients without CW. Twenty-eight of 30 patients (93%) received medical management after the index stroke (23 with antiplatelet therapy and 5 with anticoagulant therapy). During 2 years of follow-up, 5 of 30 patients (17%) with CW had a recurrent stroke compared with 5 of 168 patients (3%) without CW (adjusted hazard ratio, 4.9; 95% CI, 1.4-18.1).
Conclusions and relevance: In this study, 1 of 6 patients with a symptomatic CW had a recurrent stroke within 2 years, suggesting that medical management alone may not provide sufficient protection for patients with CW.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
