

Molecular Epidemiology, Natural History, and Long-Term Outcomes of Multidrug-Resistant Enterobacterales Colonization and Infections Among Solid Organ Transplant Recipients
- PMID: 33970222
- PMCID: PMC8834656
- DOI: 10.1093/cid/ciab427
Molecular Epidemiology, Natural History, and Long-Term Outcomes of Multidrug-Resistant Enterobacterales Colonization and Infections Among Solid Organ Transplant Recipients
Abstract
Background: Multidrug-resistant Enterobacterales (MDR-E), including carbapenem-resistant and third-generation cephalosporin-resistant Enterobacterales (CRE, CefR-E), are major pathogens following solid organ transplantation (SOT).
Methods: We prospectively studied patients who underwent lung, liver, and small bowel transplant from February 2015 through March 2017. Weekly perirectal swabs (up to 100 days post-transplant) were cultured for MDR-E. Whole-genome sequencing (WGS) was performed on gastrointestinal (GI) tract-colonizing and disease-causing isolates.
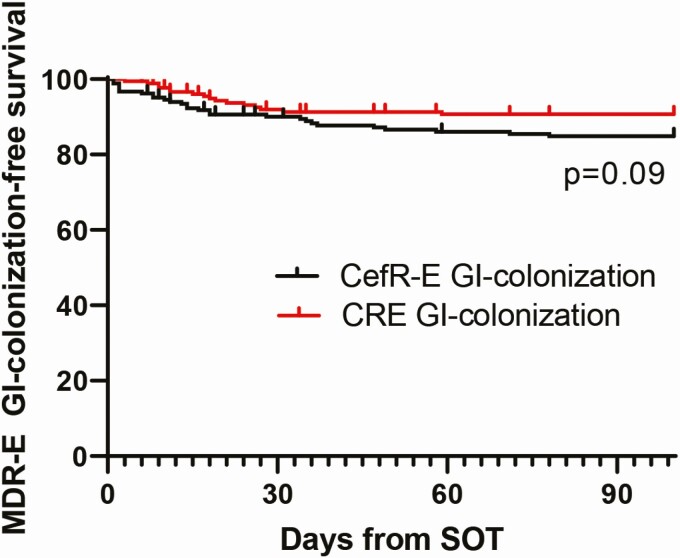
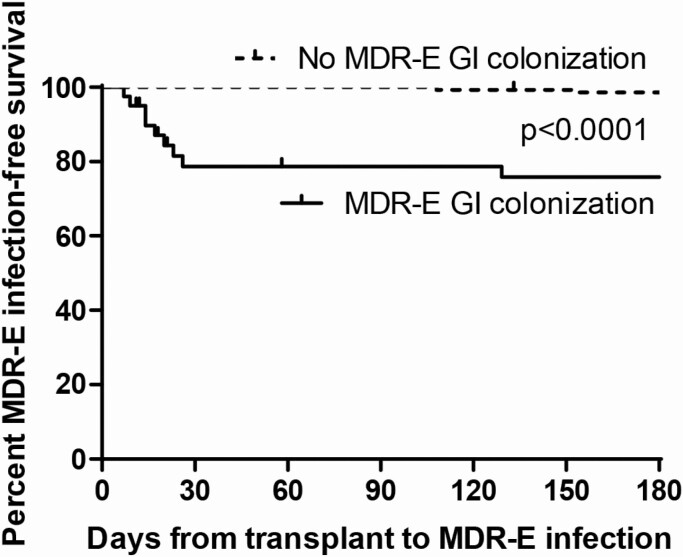
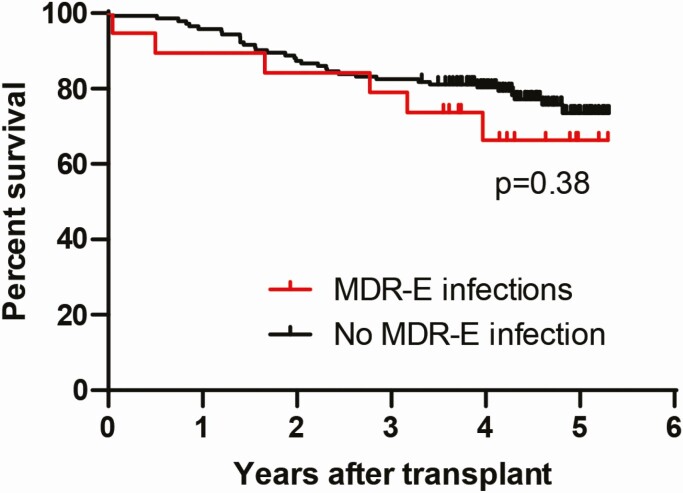
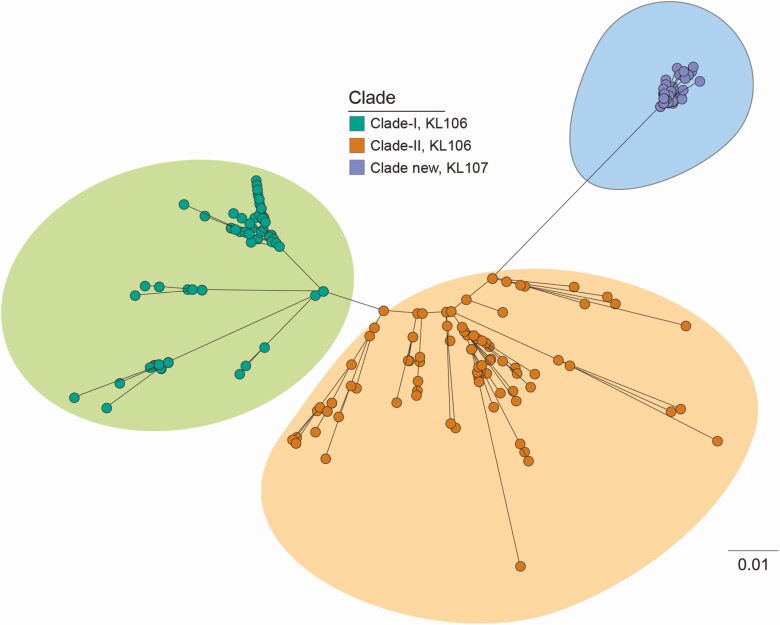
Results: Twenty-five percent (40 of 162) of patients were MDR-E GI-colonized. Klebsiella pneumoniae was the most common CRE and CefR-E. Klebsiella pneumoniae carbapenemases and CTX-M were leading causes of CR and CefR, respectively. Thirty-five percent of GI colonizers developed MDR-E infection vs 2% of noncolonizers (P < .0001). The attack rate was higher among CRE colonizers than CefR-E colonizers (53% vs 21%, P = .049). GI colonization and high body mass index were independent risk factors for MDR-E infection (P ≤ .004). Thirty-day mortality among infected patients was 6%. However, 44% of survivors developed recurrent infections; 43% of recurrences were late (285 days to 3.9 years after the initial infection). Long-term survival (median, 4.3 years post-transplant) did not differ significantly between MDR-E-infected and MDR-E-noninfected patients (71% vs 77%, P = .56). WGS phylogenetic analyses revealed that infections were caused by GI-colonizing strains and suggested unrecognized transmission of novel clonal group-258 sublineage CR-K. pneumoniae and horizontal transfer of resistance genes.
Conclusions: MDR-E GI colonization was common following SOT and predisposed patients to infections by colonizing strains. MDR-E infections were associated with low short- and long-term mortality, but recurrences were frequent and often occurred years after initial infections. Findings provide support for MDR-E surveillance in our SOT program.
Keywords: CRE colonization and infection; MDR-E colonization; MDR-E infection; molecular epidemiology; solid organ transplant.
© The Author(s) 2021. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Magiorakos AP, Srinivasan A, Carey RB, et al. . Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect 2012; 18:268–81. - PubMed
-
- Carrër A, Lassel L, Fortineau N, et al. . Outbreak of CTX-M-15-producing Klebsiella pneumoniae in the intensive care unit of a French hospital. Microb Drug Resist 2009; 15:47–54. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
