

Split Tibialis Anterior Tendon Transfer to The Peroneus Brevis or Tertius for the Treatment of Varus Foot Deformities in Children with Static Encephalopathy: A retrospective case series
- PMID: 33970577
- PMCID: PMC7434038
- DOI: 10.5435/JAAOSGlobal-D-20-00044
Split Tibialis Anterior Tendon Transfer to The Peroneus Brevis or Tertius for the Treatment of Varus Foot Deformities in Children with Static Encephalopathy: A retrospective case series
Abstract
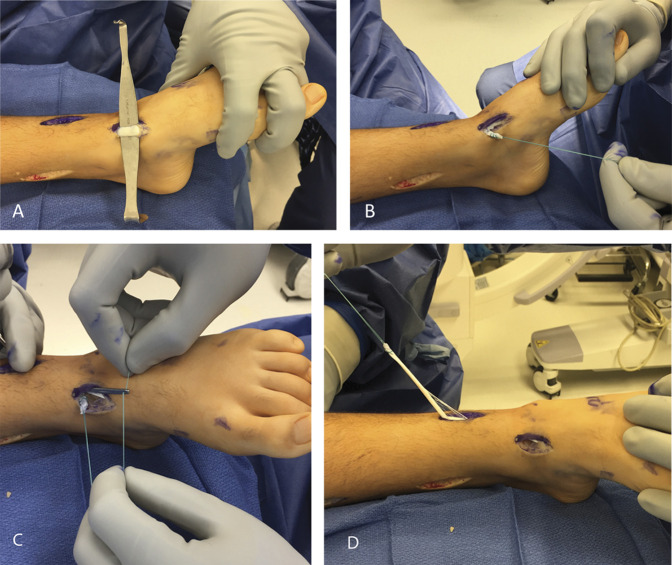
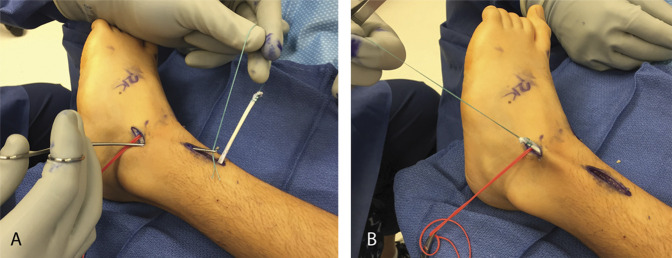
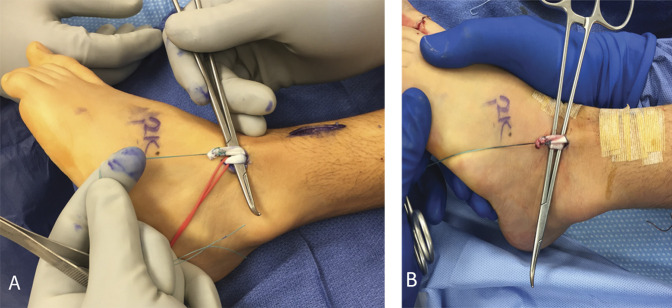
Introduction: The study purpose was to determine the safety/efficacy of a split anterior tibialis tendon transfer (SPLATT) to the peroneus tertius or brevis in children with static encephalopathy and varus feet.
Methods: A retrospective review of short- and long-term complications, change in ankle range of motion, strength, and gait kinematics. Predictors of postoperative varus or valgus were examined.
Results: One hundred thirty-three patients were included (average age [SD] 10.3 [3.7]), with an average follow-up of 3.9 (3.4) years. Forefoot/hindfoot eversion range of motion improved (P ≤ 0.05), dorsiflexor strength was maintained or improved in 76.9% of patients, and dorsiflexion in swing phase was maintained. Complications occurred in 6 of 133 patients (4.5%) and included 1 transfer failure, 1 wound dehiscence, and four pressure areas from casts. Successful correction was achieved in 77% of patients. Later onset of recurrent varus (14.4%, 10.6% requiring revision surgery) and pes valgus (8.7%, 4.8% requiring revision surgery) occurred. The length of the follow-up predicted the development of the pes valgus (odds ratio 1.28, 95% CI 1.0 to 1.6).
Discussion: SPLATT to the peroneus tertius or brevis is effective, and complications are rare. Subsequent valgus or recurrent varus deformities may occur, possibly requiring repeat surgery.
Figures


References
-
- Kay RM. Lower-extremity surgery in children with cerebral palsy, In Skaggs DL, Kocher MS, eds: Master Techniques in Orthopaedic Surgery . ed 2 Philadelphia, PA: Wolters Kluwer, 2016, pp 149-192.
-
- Wren TA, Rethlefsen S, Kay RM: Prevalence of specific gait abnormalities in children with cerebral palsy: Influence of cerebral palsy subtype, age, and previous surgery. J Pediatr Orthop 2005;25:79-83. - PubMed
-
- Michlitsch MG, Rethlefsen SA, Kay RM: The contributions of anterior and posterior tibialis dysfunction to varus foot deformity in patients with cerebral palsy. J Bone Joint Surg Am 2006;88:1764-1768. - PubMed
-
- Kuo KN, Hennigan SP, Hastings ME: Anterior tibial tendon transfer in residual dynamic clubfoot deformity. J Pediatr Orthop 2001;21:35-41. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
