

Associations of treated and untreated human papillomavirus infection with preterm delivery and neonatal mortality: A Swedish population-based study
- PMID: 33970907
- PMCID: PMC8143418
- DOI: 10.1371/journal.pmed.1003641
Associations of treated and untreated human papillomavirus infection with preterm delivery and neonatal mortality: A Swedish population-based study
Abstract
Background: Treatment of cervical intraepithelial neoplasia (CIN) is associated with an increased risk of preterm delivery (PTD) although the exact pathomechanism is not yet understood. Women with untreated CIN also seem to have an increased risk of PTD. It is unclear whether this is attributable to human papillomavirus (HPV) infection or other factors. We aimed to investigate whether HPV infection shortly before or during pregnancy, as well as previous treatment for CIN, is associated with an increased risk of PTD and other adverse obstetric and neonatal outcomes.
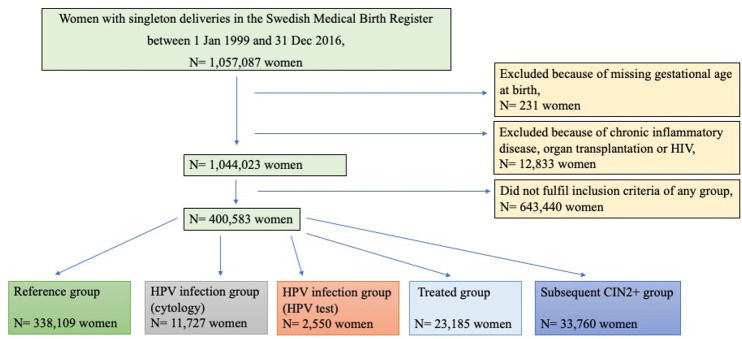
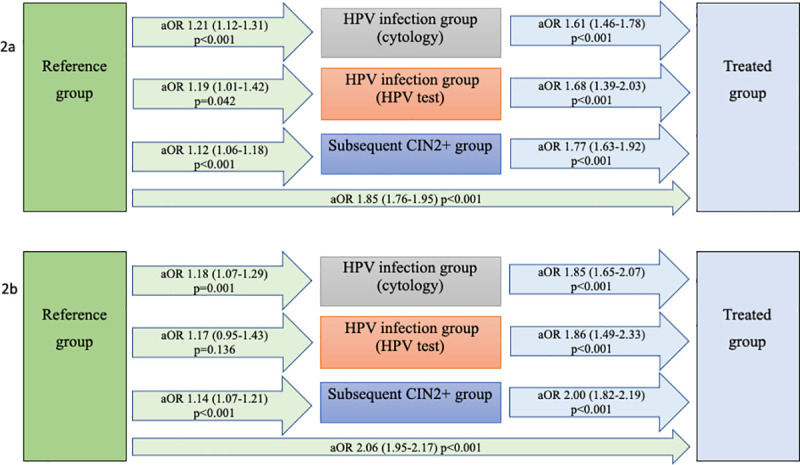
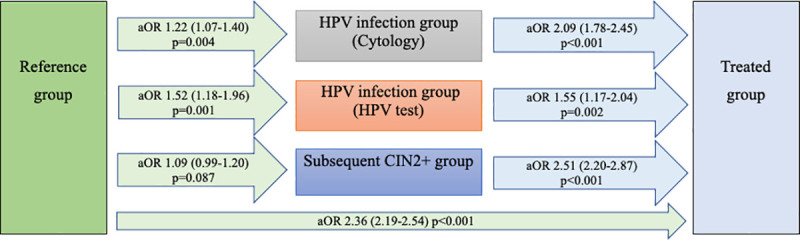
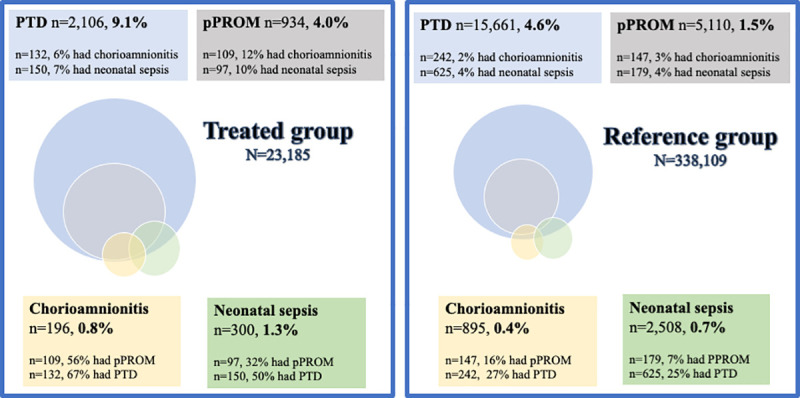
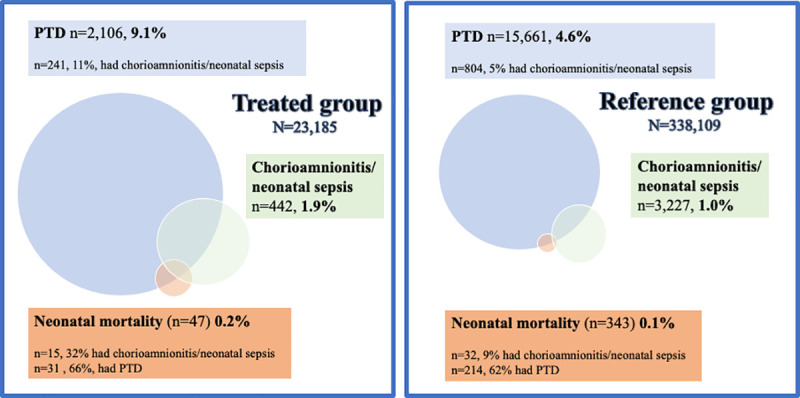
Methods and findings: This was a retrospective population-based register study of women with singleton deliveries registered in the Swedish Medical Birth Register 1999-2016 (n = 1,044,023). The study population had a mean age of 30.2 years (SD 5.2) and a mean body mass index of 25.4 kg/m2 (SD 3.0), and 44% of the women were nulliparous before delivery. Study groups were defined based on cervical HPV tests, cytology, and histology, as registered in the Swedish National Cervical Screening Registry. Women with a history of exclusively normal cytology (n = 338,109) were compared to women with positive HPV tests (n = 2,550) or abnormal cytology (n = 11,727) within 6 months prior to conception or during the pregnancy, women treated for CIN3 before delivery (n = 23,185), and women with CIN2+ diagnosed after delivery (n = 33,760). Study groups were compared concerning obstetric and neonatal outcomes by logistic regression, and comparisons were adjusted for socioeconomic and health-related confounders. HPV infection was associated with PTD (adjusted odds ratio [aOR] 1.19, 95% CI 1.01-1.42, p = 0.042), preterm prelabor rupture of membranes (pPROM) (aOR 1.52, 95% CI 1.18-1.96, p < 0.001), prelabor rupture of membranes (PROM) (aOR 1.24, 95% CI 1.08-1.42, p = 0.002), and neonatal mortality (aOR 2.69, 95% CI 1.25-5.78, p = 0.011). Treatment for CIN was associated with PTD (aOR 1.85, 95% CI 1.76-1.95, p < 0.001), spontaneous PTD (aOR 2.06, 95% CI 1.95-2.17, p < 0.001), pPROM (aOR 2.36, 95% CI 2.19-2.54, p < 0.001), PROM (aOR 1.11, 95% CI 1.05-1.17, p < 0.001), intrauterine fetal death (aOR 1.35, 95% CI 1.05-1.72, p = 0.019), chorioamnionitis (aOR 2.75, 95% CI 2.33-3.23, p < 0.001), intrapartum fever (aOR 1.24, 95% CI 1.07-1.44, p = 0.003), neonatal sepsis (aOR 1.55, 95% CI 1.37-1.75, p < 0.001), and neonatal mortality (aOR 1.79, 95% CI 1.30-2.45, p < 0.001). Women with CIN2+ diagnosed within 3 years after delivery had increased PTD risk (aOR 1.18, 95% CI 1.10-1.27, p < 0.001). Limitations of the study include the retrospective design and the fact that because HPV test results only became available in 2007, abnormal cytology was used as a proxy for HPV infection.
Conclusions: In this study, we found that HPV infection shortly before or during pregnancy was associated with PTD, pPROM, PROM, and neonatal mortality. Previous treatment for CIN was associated with even greater risks for PTD and pPROM and was also associated with PROM, neonatal mortality, and maternal and neonatal infectious complications.
Conflict of interest statement
I have read the journal´s policy and the authors of this manuscript have the following competing interests: CK has research grants for clinical trial Assar Gabrielsson’s Foundation for Cancer-Related Clinical Research, Hjalmar Svensson’s Research Foundation. She is presently head of one Swedish site of a multicenter international academic clinical HPV-vaccine trial where the sponsor, Imperial College, London, receive some support from MSD. She is a member of the Screening and colposcopy national guidelines committee, and she is the secretary of The Swedish Society for Colposcopy and Cervical Cancer Prevention/C-ARG. She has received reimbursement from Gedeon Richter for lectures on meeting arranged by the company. BS has research grants for clinical trial by the Governmental agreement with Swedish counties, ALF, and by the Region of Västra Götaland. He is presently Swedish head of an multicenter international academic clinical HPV-vaccine trial where the sponsor, Imperial College, London, receive some support from MSD. The past five years he has served as chairman of the Swedish Cervical screening coordinating committee, as chairman of the Screening and colposcopy national guidelines committee, and as head of the Cervical screening process register. He has been a member of the National Board of health and welfare evaluation committee for the Cervical screening program. He has received no financial support or reimbursement from commercial companies for any activity. BJ has research grants from the Swedish Research Council, the Research Council of Norway, the March of Dimes, and the Burroughs Wellcome Fund. During the last five years, he has performed clinical diagnostic trials for Ariosa, Natera, Vanadis, and Hologic with reimbursement costs per recruited patient. He has conducted clinical trials on probiotics in pregnancy in collaboration with BioGaia and FukoPharma. He has also been involved in the IMPACT study where Roche and Thermo Fisher paid for PLGF-analyzes. He has also arranged scientific meetings with commercial partners (ESPBC 2016) and a Nordic educational meeting on NIPT and preeclampsia screening (2017). No lectures, travel, or personal reimbursements from the companies.
Figures
References
-
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. IARC monographs on the evaluation of carcinogenic risks to humans. Volume 90. Human papillomaviruses. Lyon: International Agency for Research on Cancer; 2007.
-
- Ferrero DM, Larson J, Jacobsson B, Di Renzo GC, Norman JE, Martin JN Jr, et al. Cross-country individual participant analysis of 4.1 million singleton births in 5 countries with very high human development index confirms known associations but provides no biologic explanation for 2/3 of all preterm births. PLoS ONE. 2016;11(9):e0162506. 10.1371/journal.pone.0162506 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
