

18F-fluciclovine-PET/CT imaging versus conventional imaging alone to guide postprostatectomy salvage radiotherapy for prostate cancer (EMPIRE-1): a single centre, open-label, phase 2/3 randomised controlled trial
- PMID: 33971152
- PMCID: PMC8279109
- DOI: 10.1016/S0140-6736(21)00581-X
18F-fluciclovine-PET/CT imaging versus conventional imaging alone to guide postprostatectomy salvage radiotherapy for prostate cancer (EMPIRE-1): a single centre, open-label, phase 2/3 randomised controlled trial
Abstract
Background: Molecular imaging is increasingly used to guide treatment decisions and planning in prostate cancer. We aimed to evaluate the role of 18F-fluciclovine-PET/CT in improving cancer control compared with conventional imaging (bone scan and either CT or MRI) alone for salvage postprostatectomy radiotherapy.
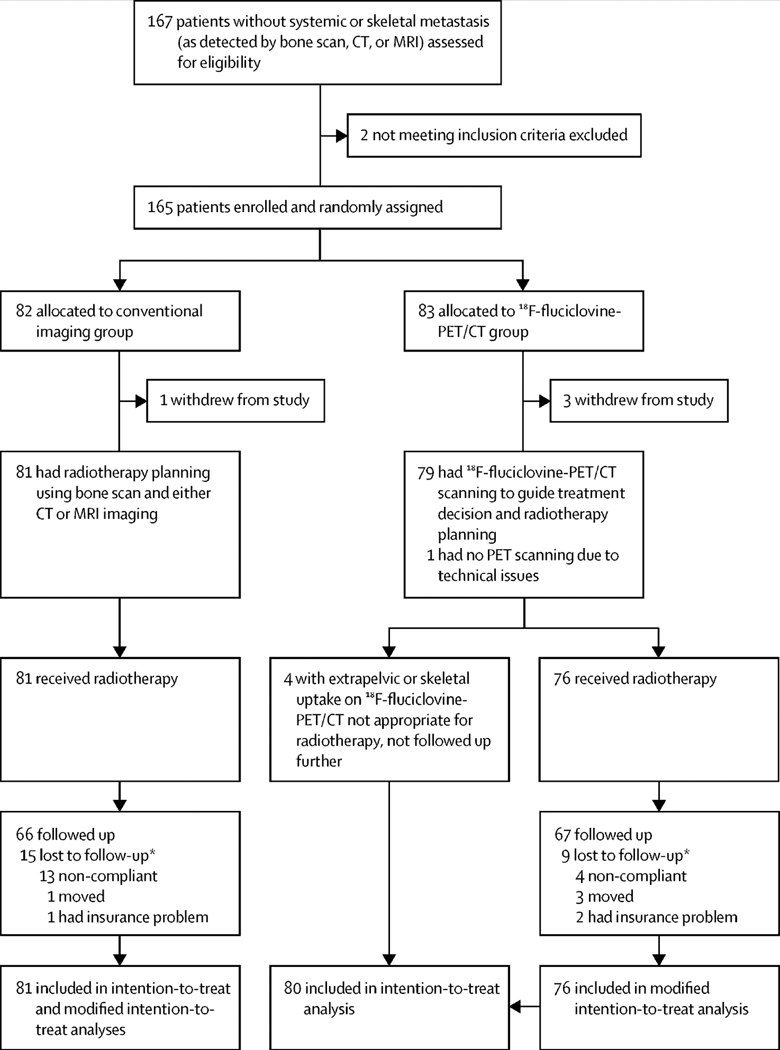
Methods: In EMPIRE-1, a single-centre, open-label, phase 2/3 randomised controlled trial, patients with prostate cancer with detectable PSA after prostatectomy and negative conventional imaging (no extrapelvic or bone findings) were randomly assigned in a 1:1 ratio to radiotherapy directed by conventional imaging alone or to conventional imaging plus 18F-fluciclovine-PET/CT. Computer-generated randomisation was stratified by PSA concentration, adverse pathology indicators, and androgen deprivation therapy intent. In the 18F-fluciclovine-PET/CT group, radiotherapy decisions were rigidly determined by PET findings, which were also used for target delineation. The primary endpoint was 3 year event-free survival, with events defined as biochemical or clinical recurrence or progression, or initiation of systemic therapy, using univariate and multivariable analyses in patients who received radiotherapy. This trial is registered with ClinicalTrials.gov, NCT01666808 and is closed to new participants.
Findings: From Sept 18, 2012, to March 4, 2019, 165 patients were randomly assigned, with median follow-up of 3·52 years (95% CI 2·98-3·95). PET findings resulted in four patients in the 18F-fluciclovine-PET/CT group having radiotherapy aborted; these patients were excluded from survival analyses. Median survival was not reached (95% CI 35·2-not reached; 33% of 81 patients had events) in the conventional imaging group compared with not reached (95% CI not reached-not reached; 20% of 76 patients) in the 18F-fluciclovine-PET/CT group, and 3 year event-free survival was 63·0% (95% CI 49·2-74·0) in the conventional imaging group versus 75·5% (95% CI 62·5-84·6) for 18F-fluciclovine-PET/CT (difference 12·5; 95% CI 4·3-20·8; p=0·0028). In adjusted analyses, study group (hazard ratio 2·04 [95% CI 1·06-3·93], p=0·0327) was significantly associated with event-free survival. Toxicity was similar in both study groups, with the most common adverse events being late urinary frequency or urgency (37 [46%] of 81 patients in the conventional imaging group and 31 [41%] of 76 in the PET group), and acute diarrhoea (11 [14%] in the conventional imaging group and 16 [21%] in the PET group).
Interpretation: Inclusion of 18F-fluciclovine-PET into postprostatectomy radiotherapy decision making and planning significantly improved survival free from biochemical recurrence or persistence. Integration of novel PET radiotracers into radiotherapy decisions and planning for prostate cancer patients warrants further study.
Funding: National Institutes of Health/National Cancer Institute, Blue Earth Diagnostics, and Winship Cancer Institute of Emory University.
Copyright © 2021 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests ABJ reports personal fees from Blue Earth Diagnostics for advisory board services outside the submitted work. MG is entitled to a royalty derived from sale of products related to the research described in this report. The terms of this arrangement have been reviewed and approved by Emory University in accordance with its conflict of interest policies. The research consent forms state that he is entitled to a share of sales royalty received by Emory University from Nihon MediPhysics under that agreement. The terms of this arrangement have been reviewed and approved by Emory University in accordance with its conflict of interest policies. DMS participates through the Emory University Office of Sponsored Projects in sponsored grants including those funded or partially funded by Blue Earth Diagnostics, Nihon MediPhysics, Telix Pharmaceuticals (US), Advanced Accelerator Applications, FUJIFILM Pharmaceuticals USA, and Amgen. DMS also reports consultant fees outside the submitted work from Syncona, AIM Specialty Health, Global Medical Solutions Taiwan, and Progenics Pharmaceuticals. The other authors declare no competing interests.
Figures

Comment in
-
Beyond the AJR: Integrating 18F-Fluciclovine PET/CT Into Salvage Radiotherapy Planning for Recurrent Prostate Cancer Reduces Rates of Biochemical Failure (EMPIRE-1 Trial).AJR Am J Roentgenol. 2022 Mar;218(3):559. doi: 10.2214/AJR.21.26599. Epub 2021 Aug 4. AJR Am J Roentgenol. 2022. PMID: 34346784 No abstract available.
References
-
- Jani AB, Hellman S. Early prostate cancer: clinical decision-making. Lancet 2003; 361; 1045–53. - PubMed
-
- Hamdy FC, Donovan JL, Lane JA, et al. 10-Year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N Engl J Med 2016; 375: 1415–24. - PubMed
-
- Freedland SJ, Humphreys EB, Mangold LA et al. Risk of prostate cancer-specific mortality following biochemical recurrence after radical prostatectomy. JAMA 2005; 294: 433–9. - PubMed
-
- Bolla M, van Poppel H, Tombal B, et al. Postoperative radiotherapy after radical prostatectomy for high-risk prostate cancer: long-term results of a randomised controlled trial (EORTC trial 22911). Lancet 2012; 380: 2018–27. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
