

Association Between β-Blockers and Outcomes in Heart Failure With Preserved Ejection Fraction: Current Insights From the SwedeHF Registry
- PMID: 33971289
- PMCID: PMC8573055
- DOI: 10.1016/j.cardfail.2021.04.015
Association Between β-Blockers and Outcomes in Heart Failure With Preserved Ejection Fraction: Current Insights From the SwedeHF Registry
Abstract
Background: β-Blockers have an uncertain effect in heart failure with a preserved ejection fraction of 50% or higher (heart failure with preserved ejection fraction [HFpEF]).
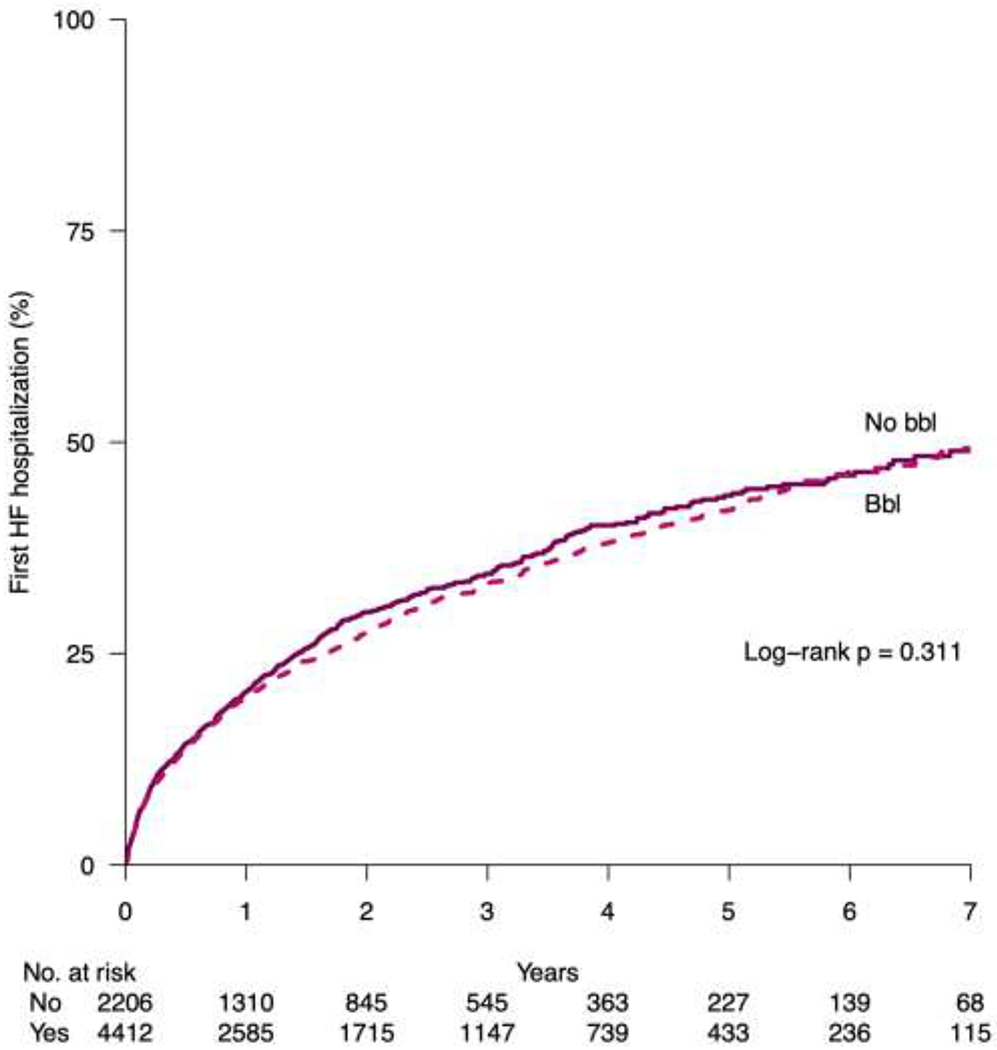
Methods and results: We included patients with HFpEF from the Swedish Heart Failure Registry (SwedeHF) enrolled from 2011 through 2018. In a 2:1 propensity-score matched analysis (β-blocker use vs nonuse), we assessed the primary outcome first HF hospitalization, the coprimary outcome cardiovascular (CV) death, and the secondary outcomes of all-cause hospitalization and all-cause death. We performed intention-to-treat and a per-protocol consistency analyses. There were a total of 14,434 patients (median age 79 years, IQR 71-85 years, 51% women); 80% were treated with a β-blocker at baseline. Treated patients were younger and had higher rates of atrial fibrillation and coronary artery disease, and higher N-terminal pro-B-type natriuretic peptide levels. In the 4412:2206 patient matched cohort, at 5 years, 42% (95% CI 40%-44%) vs 44% (95% CI 41%-47%) had a HF admission and 38% (IQR 36%-40%) vs 40% (IQR 36%-42%) died from CV causes. In the intention-to-treat analysis, β-blocker use was not associated with HF admissions (hazard ratio 0.95 [95% CI 0.87-1.05, P = .31]) or CV death (hazard ratio 0.94 [95% CI 0.85-1.03, P = .19]). In the subgroup analyses, men seemed to have a more favorable association between β-blockers and outcomes than did women. There were no associations between β-blocker use and secondary outcomes.
Conclusions: In patients with HFpEF, β-blocker use is common but not associated with changes in HF hospitalization or cardiovascular mortality. In the absence of a strong rational and randomized control trials the case for β-blockers in HFpEF remains inconclusive.
Bullet points: ● The effect of β-blockers with heart failure with preserved ejection fraction of 50% or greater is uncertain.● In a propensity score-matched heart failure with preserved ejection fraction analysis in the SwedeHF registry, β-blockers were not associated with a change in risk for heart failure admissions or cardiovascular deaths.
Lay summary: The optimal treatment for heart failure with a preserved pump function remains unknown. Despite the lack of scientific studies, β-blockers are very commonly used. When matching patients with a similar risk profile in a large heart failure registry, the use of β-blockers for the treatment of heart failure with a preserved pump function was not associated with any changes in heart failure hospital admissions or cardiovascular death.
Copyright © 2021 Elsevier Inc. All rights reserved.
Figures


References
-
- Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Drazner MH, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2013;128(16):e240–327. - PubMed
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med. 2006;355(3):251–9. - PubMed
-
- Lewis EF, Lamas GA, O’Meara E, Granger CB, Dunlap ME, McKelvie RS, et al. Characterization of health-related quality of life in heart failure patients with preserved versus low ejection fraction in CHARM. Eur J Heart Fail. 2007;9(1):83–91. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
