

Suppression of cancer-associated bone loss through dynamic mechanical loading
- PMID: 33971314
- PMCID: PMC10044486
- DOI: 10.1016/j.bone.2021.115998
Suppression of cancer-associated bone loss through dynamic mechanical loading
Abstract
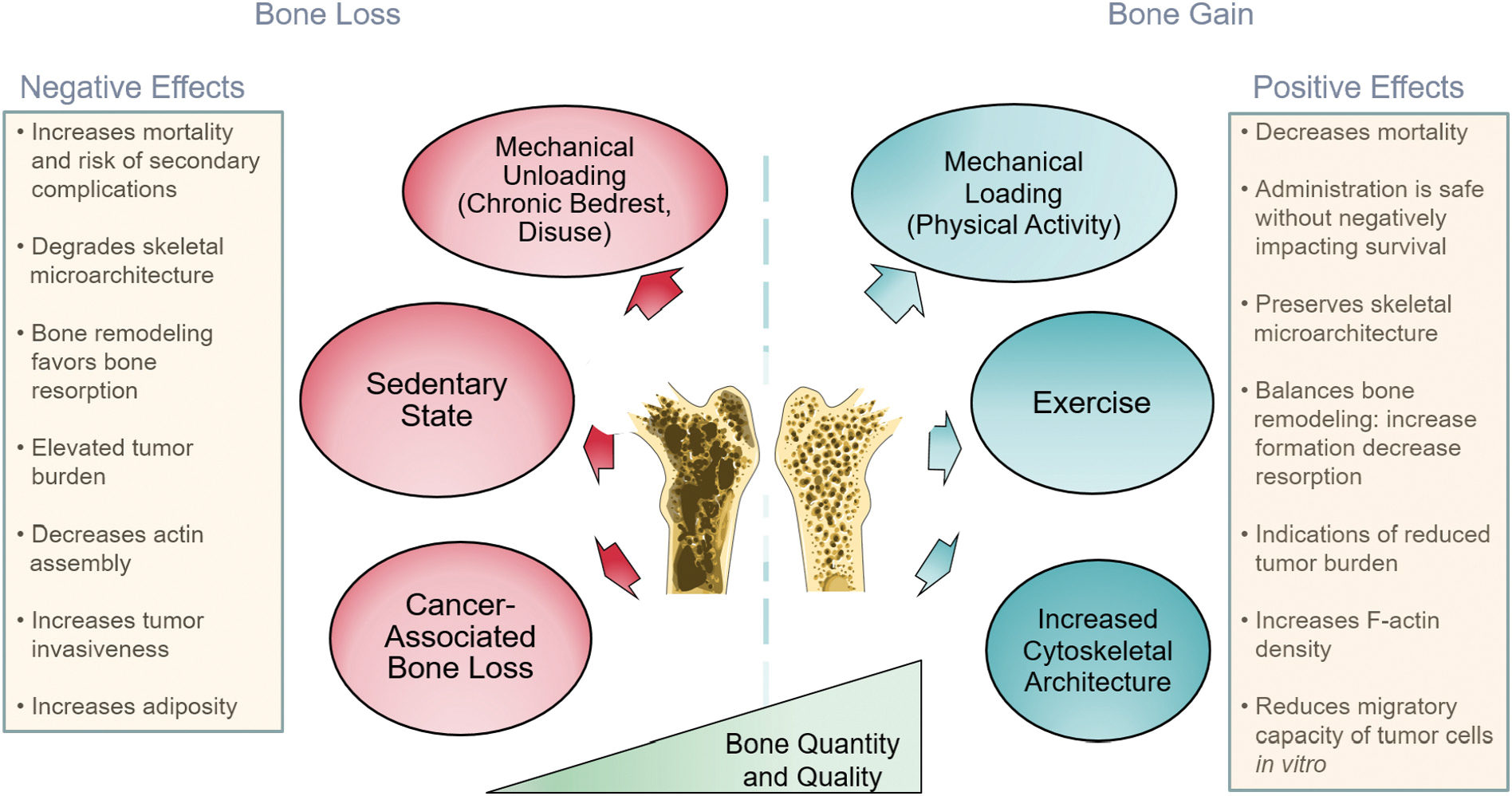
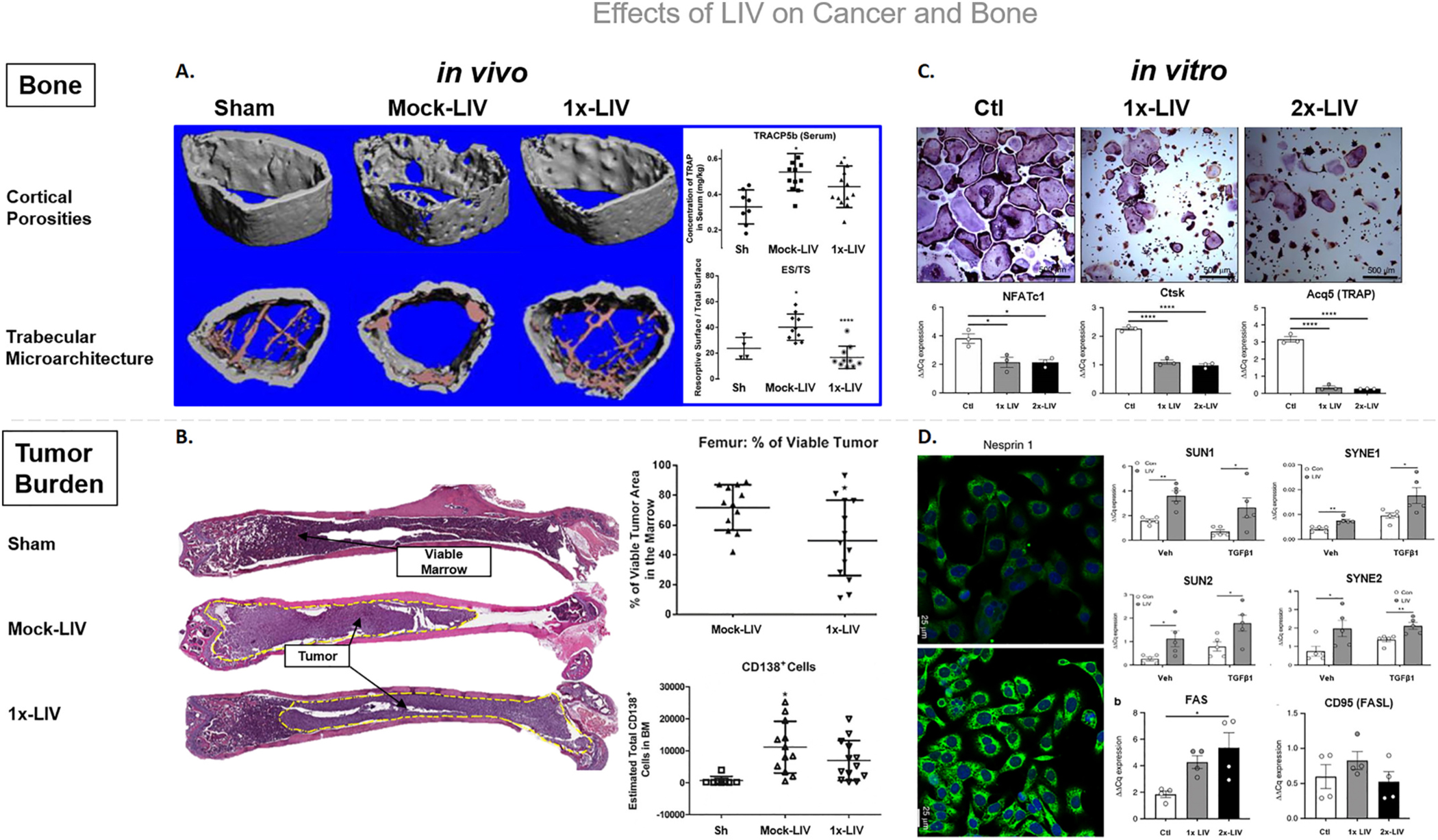
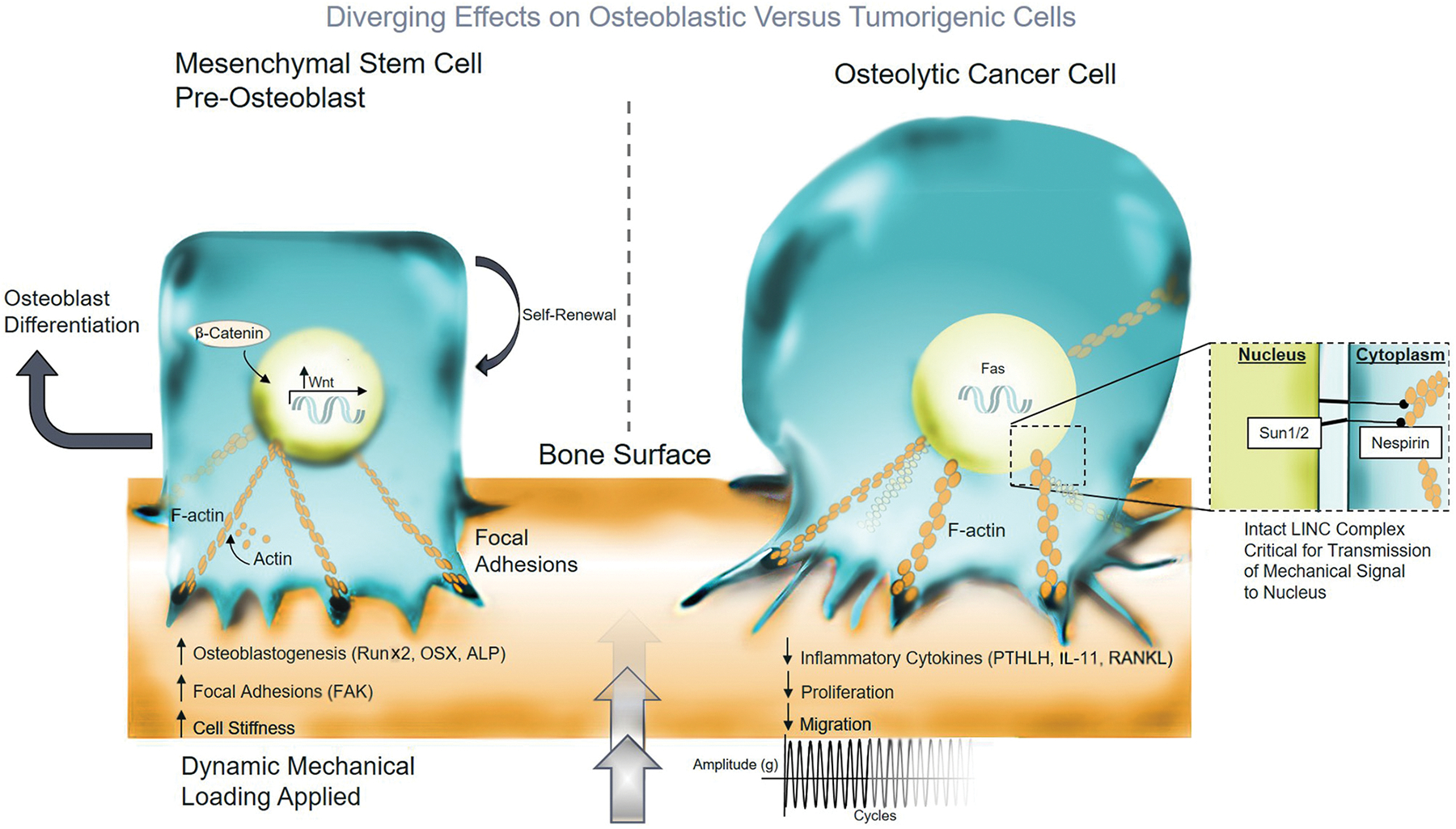
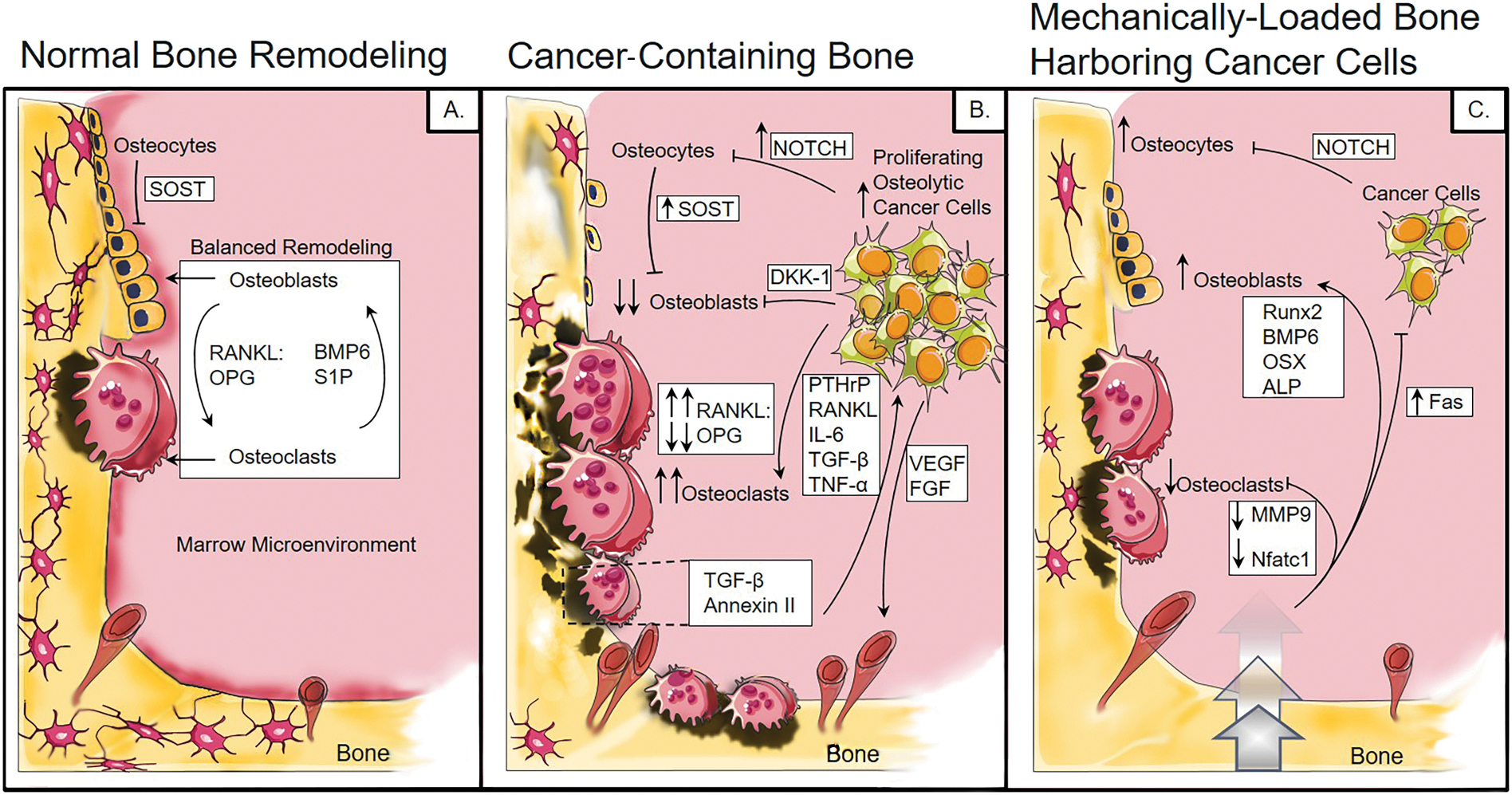
Patients afflicted with or being treated for cancer constitute a distinct and alarming subpopulation who exhibit elevated fracture risk and heightened susceptibility to developing secondary osteoporosis. Cancer cells uncouple the regulatory processes central for the adequate regulation of musculoskeletal tissue. Systemically taxing treatments to target tumors or disrupt the molecular elements driving tumor growth place considerable strain on recovery efforts. Skeletal tissue is inherently sensitive to mechanical forces, therefore attention to exercise and mechanical loading as non-pharmacological means to preserve bone during treatment and in post-treatment rehabilitative efforts have been topics of recent focus. This review discusses the dysregulation that cancers and the ensuing metabolic dysfunction that confer adverse effects on musculoskeletal tissues. Additionally, we describe foundational mechanotransduction pathways and the mechanisms by which they influence both musculoskeletal and cancerous cells. Functional and biological implications of mechanical loading at the tissue and cellular levels will be discussed, highlighting the current understanding in the field. Herein, in vitro, translational, and clinical data are summarized to consider the positive impact of exercise and low magnitude mechanical loading on tumor-bearing skeletal tissue.
Keywords: Bone remodeling; Breast cancer bone metastases; Cancer-associated bone disease; Low intensity vibrations; Low magnitude mechanical signals; Mechanical loading; Multiple myeloma; Osteolytic lesions.
Copyright © 2021. Published by Elsevier Inc.
Conflict of interest statement
Declaration of competing interest
C.T. Rubin is a founder of Marodyne Medical, LLC. and Lahara Bio, a developer of LIV technology, and has several patents issued and pending related to the ability of mechanical signals to control musculoskeletal and metabolic disorders. The authors declare that information was gathered for this review manuscript in the absence of any commercial or financial relationships that could be construed as a potential conflict-of-interest.
Figures
Similar articles
-
Low-level mechanical signals and their potential as a non-pharmacological intervention for osteoporosis.Age Ageing. 2006 Sep;35 Suppl 2:ii32-ii36. doi: 10.1093/ageing/afl082. Age Ageing. 2006. PMID: 16926201
-
Mechanotransduction in musculoskeletal tissue regeneration: effects of fluid flow, loading, and cellular-molecular pathways.Biomed Res Int. 2014;2014:863421. doi: 10.1155/2014/863421. Epub 2014 Aug 18. Biomed Res Int. 2014. PMID: 25215295 Free PMC article. Review.
-
Bone's Response to Mechanical Loading in Aging and Osteoporosis: Molecular Mechanisms.Calcif Tissue Int. 2020 Oct;107(4):301-318. doi: 10.1007/s00223-020-00724-0. Epub 2020 Jul 24. Calcif Tissue Int. 2020. PMID: 32710266 Review.
-
Muscle forces or gravity: what predominates mechanical loading on bone?Med Sci Sports Exerc. 2009 Nov;41(11):2050-5. doi: 10.1249/MSS.0b013e3181a8c717. Med Sci Sports Exerc. 2009. PMID: 19812511 Free PMC article.
-
Dynamic hydraulic fluid stimulation regulated intramedullary pressure.Bone. 2013 Nov;57(1):137-41. doi: 10.1016/j.bone.2013.07.030. Epub 2013 Jul 27. Bone. 2013. PMID: 23895997 Free PMC article.
Cited by
-
Antitumoral-Embedded Biopolymeric Spheres for Implantable Devices.Pharmaceutics. 2024 Jun 3;16(6):754. doi: 10.3390/pharmaceutics16060754. Pharmaceutics. 2024. PMID: 38931875 Free PMC article.
-
Anticancer Peptides Derived from Aldolase A and Induced Tumor-Suppressing Cells Inhibit Pancreatic Ductal Adenocarcinoma Cells.Pharmaceutics. 2023 Oct 11;15(10):2447. doi: 10.3390/pharmaceutics15102447. Pharmaceutics. 2023. PMID: 37896207 Free PMC article.
-
Prognostic value of preoperative low bone mineral density in patients with digestive cancers: a systematic review and meta-analysis.Arch Osteoporos. 2022 Feb 11;17(1):33. doi: 10.1007/s11657-022-01060-6. Arch Osteoporos. 2022. PMID: 35149903 Free PMC article.
-
Integrating molecular biomarkers in breast cancer rehabilitation. What is the current evidence? A systematic review of randomized controlled trials.Front Mol Biosci. 2022 Sep 8;9:930361. doi: 10.3389/fmolb.2022.930361. eCollection 2022. Front Mol Biosci. 2022. PMID: 36158576 Free PMC article. Review.
-
Cellulose nanofiber reinforced curcumin-infused calcium phosphate silicate cement for various bone-tissue engineering application.Front Oncol. 2025 Jan 14;14:1516638. doi: 10.3389/fonc.2024.1516638. eCollection 2024. Front Oncol. 2025. PMID: 39876894 Free PMC article.
References
-
- Black DM, Rosen CJ, Postmenopausal osteoporosis, N. Engl. J. Med. 374 (3) (2016) 254–262. - PubMed
-
- Coleman RE, Skeletal complications of malignancy, Cancer 80 (8) (1997) 1588–1594. - PubMed
-
- Saad F, et al., Pathologic fractures correlate with reduced survival in patients with malignant bone disease, Cancer 110 (8) (2007) 1860–1867. - PubMed
-
- Guise TA, Bone loss and fracture risk associated with cancer therapy, Oncologist 11 (10) (2006) 1121–1131. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
