

Morphology-based radiomics signature: a novel determinant to identify multiple intracranial aneurysms rupture
- PMID: 33971625
- PMCID: PMC8148474
- DOI: 10.18632/aging.203001
Morphology-based radiomics signature: a novel determinant to identify multiple intracranial aneurysms rupture
Abstract
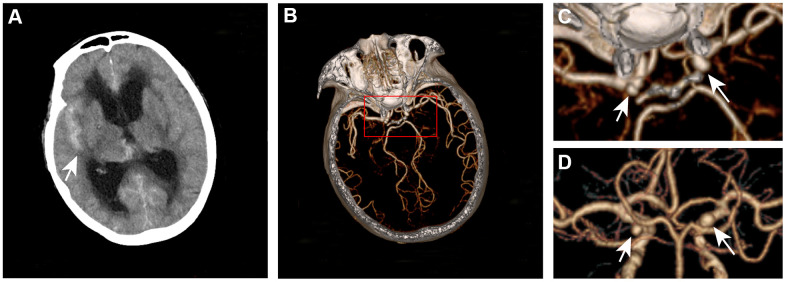
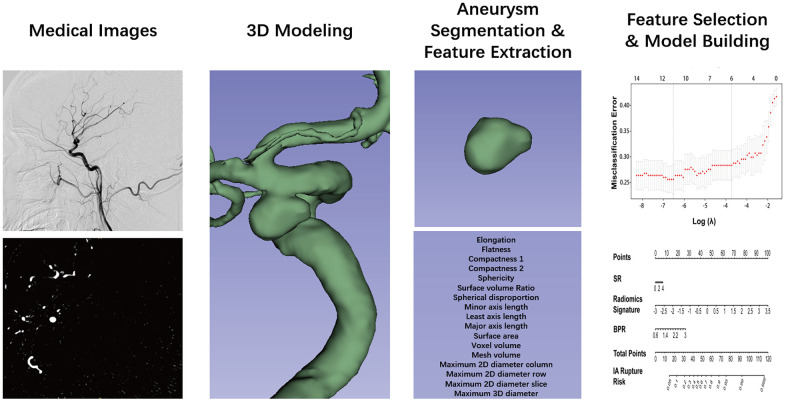
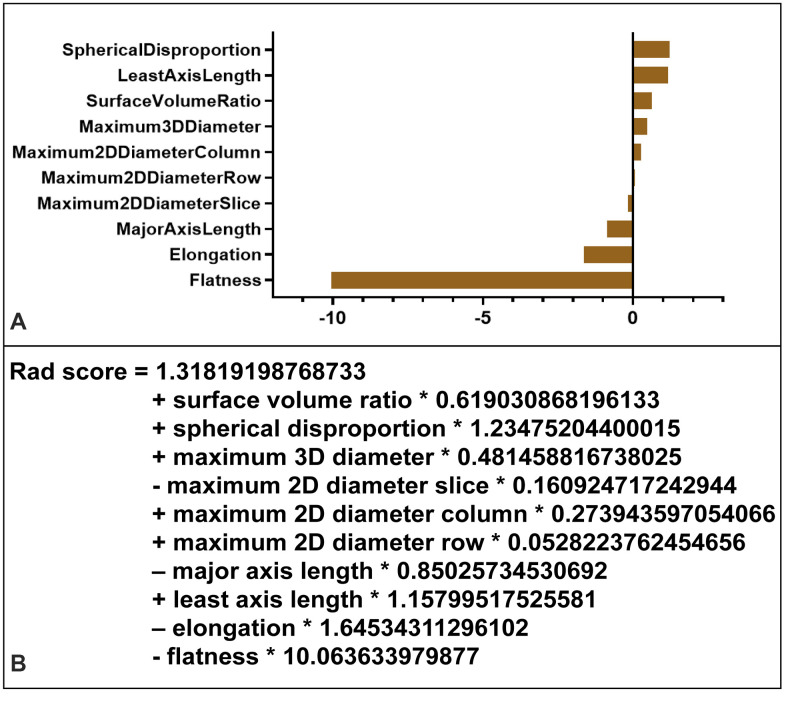
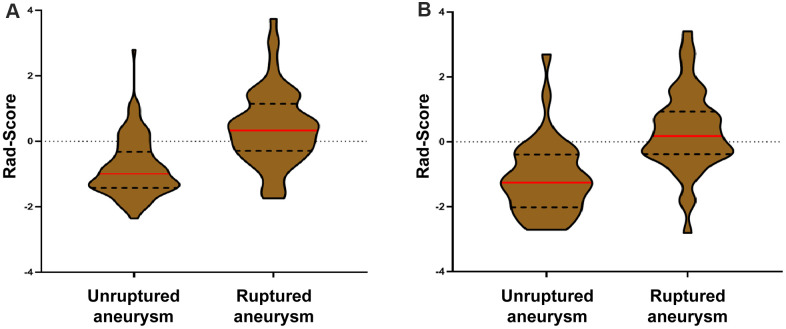
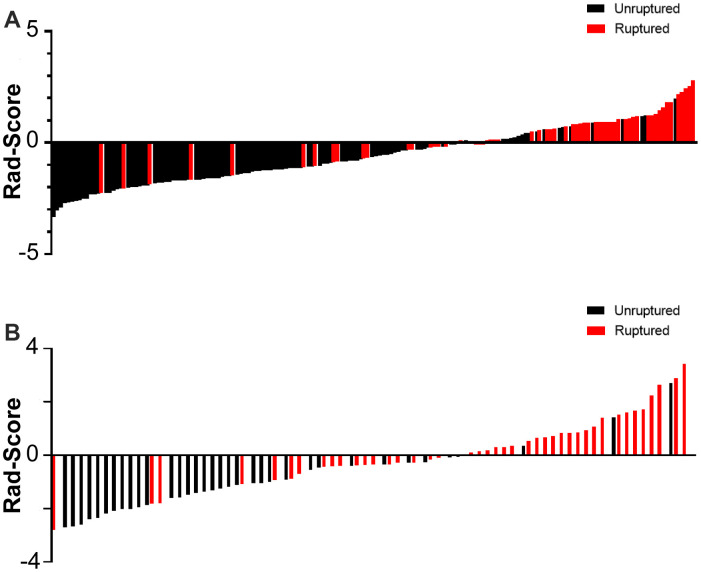
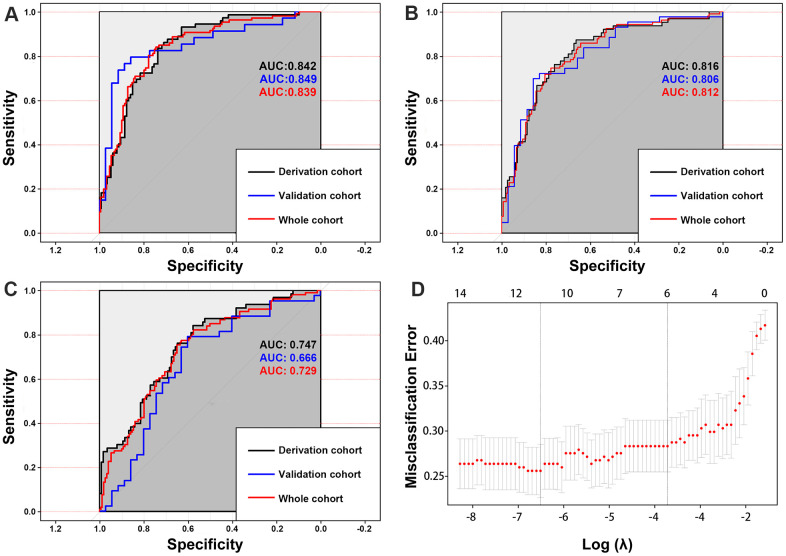
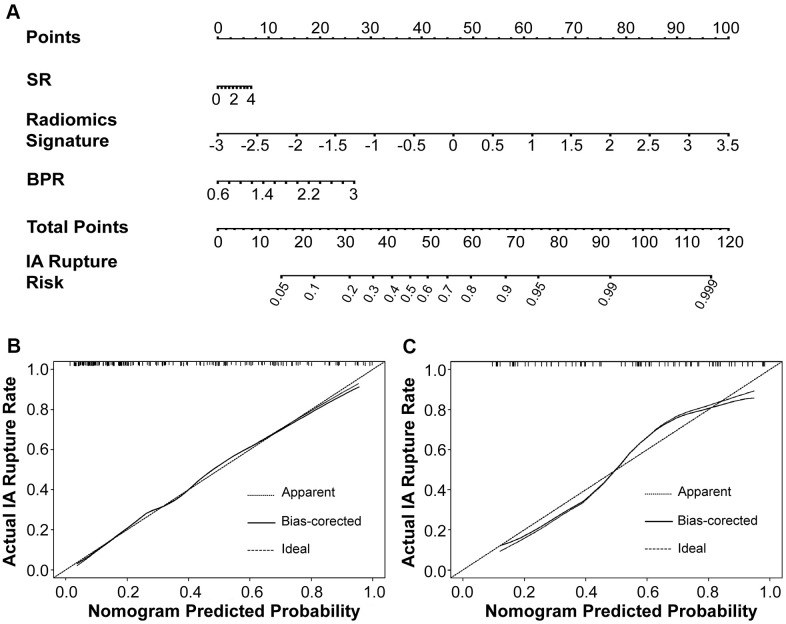
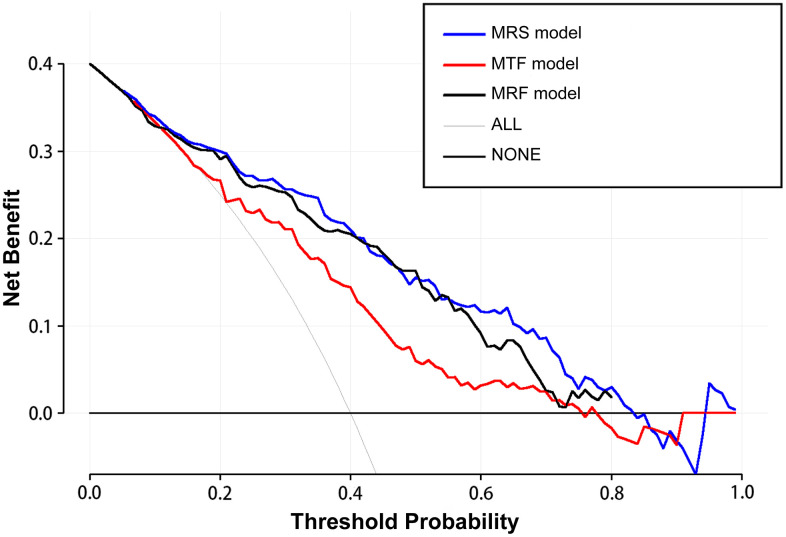
We aimed to develop and validate a morphology-based radiomics signature nomogram for assessing the risk of intracranial aneurysm (IA) rupture. A total of 254 aneurysms in 105 patients with subarachnoid hemorrhage and multiple intracranial aneurysms from three centers were retrospectively reviewed and randomly divided into the derivation and validation cohorts. Radiomics morphological features were automatically extracted from digital subtraction angiography and selected by the least absolute shrinkage and selection operator algorithm to develop a radiomics signature. A radiomics signature-based nomogram was developed by incorporating the signature and traditional morphological features. The performance of calibration, discrimination, and clinical usefulness of the nomogram was assessed. Ten radiomics morphological features were selected to build the radiomics signature model, which showed better discrimination with an area under the curve (AUC) equal to 0.814 and 0.835 in the derivation and validation cohorts compared with 0.747 and 0.666 in the traditional model, which only include traditional morphological features. When radiomics signature and traditional morphological features were combined, the AUC increased to 0.842 and 0.849 in the derivation and validation cohorts, thus showing better performance in assessing aneurysm rupture risk. This novel model could be useful for decision-making and risk stratification for patients with IAs.
Keywords: intracranial aneurysm; nomogram; radiomics features; radiomics signature; risk prediction.
Conflict of interest statement
Figures
Similar articles
-
A CT-based radiomics nomogram for differentiation of renal angiomyolipoma without visible fat from homogeneous clear cell renal cell carcinoma.Eur Radiol. 2020 Feb;30(2):1274-1284. doi: 10.1007/s00330-019-06427-x. Epub 2019 Sep 10. Eur Radiol. 2020. PMID: 31506816
-
A clinical-radiomics nomogram for the preoperative prediction of lung metastasis in colorectal cancer patients with indeterminate pulmonary nodules.Eur Radiol. 2019 Jan;29(1):439-449. doi: 10.1007/s00330-018-5539-3. Epub 2018 Jun 12. Eur Radiol. 2019. PMID: 29948074
-
A CT-based radiomics nomogram for differentiation of focal nodular hyperplasia from hepatocellular carcinoma in the non-cirrhotic liver.Cancer Imaging. 2020 Feb 24;20(1):20. doi: 10.1186/s40644-020-00297-z. Cancer Imaging. 2020. PMID: 32093786 Free PMC article.
-
A radiomics nomogram for preoperative prediction of microvascular invasion risk in hepatitis B virus-related hepatocellular carcinoma.Diagn Interv Radiol. 2018 May-Jun;24(3):121-127. doi: 10.5152/dir.2018.17467. Diagn Interv Radiol. 2018. PMID: 29770763 Free PMC article.
-
Establishment and multicenter external validation of a risk prediction model for de novo intracranial aneurysms based on a systematic review and meta-analysis of 19 cohorts.J Neurosurg. 2023 Sep 8;140(3):783-791. doi: 10.3171/2023.7.JNS23749. Print 2024 Mar 1. J Neurosurg. 2023. PMID: 37724813
Cited by
-
Radiomics Features on Computed Tomography Combined With Clinical-Radiological Factors Predicting Progressive Hemorrhage of Cerebral Contusion.Front Neurol. 2022 Jun 14;13:839784. doi: 10.3389/fneur.2022.839784. eCollection 2022. Front Neurol. 2022. PMID: 35775053 Free PMC article.
-
Development of a non-contrast CT-based radiomics nomogram for early prediction of delayed cerebral ischemia in aneurysmal subarachnoid hemorrhage.BMC Med Imaging. 2025 May 23;25(1):182. doi: 10.1186/s12880-025-01722-0. BMC Med Imaging. 2025. PMID: 40410679 Free PMC article.
-
Development and External Validation of a Dynamic Nomogram With Potential for Risk Assessment of Ruptured Multiple Intracranial Aneurysms.Front Neurol. 2022 Feb 8;13:797709. doi: 10.3389/fneur.2022.797709. eCollection 2022. Front Neurol. 2022. PMID: 35211083 Free PMC article.
-
Predicting the rupture status of small middle cerebral artery aneurysms using random forest modeling.Front Neurol. 2022 Jul 28;13:921404. doi: 10.3389/fneur.2022.921404. eCollection 2022. Front Neurol. 2022. PMID: 35968311 Free PMC article.
-
Application of zone classification in multiple intracranial aneurysmal subarachnoid hemorrhage treatment strategies.Heliyon. 2024 Feb 22;10(5):e26857. doi: 10.1016/j.heliyon.2024.e26857. eCollection 2024 Mar 15. Heliyon. 2024. PMID: 38434361 Free PMC article.
References
-
- Jabbarli R, Dinger TF, Darkwah Oppong M, Pierscianek D, Dammann P, Wrede KH, Kaier K, Köhrmann M, Forsting M, Kleinschnitz C, Sure U. Risk Factors for and Clinical Consequences of Multiple Intracranial Aneurysms: A Systematic Review and Meta-Analysis. Stroke. 2018; 49:848–55. 10.1161/STROKEAHA.117.020342 - DOI - PubMed
-
- Molyneux AJ, Kerr RS, Yu LM, Clarke M, Sneade M, Yarnold JA, Sandercock P, and International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, rebleeding, subgroups, and aneurysm occlusion. Lancet. 2005; 366:809–17. 10.1016/S0140-6736(05)67214-5 - DOI - PubMed
-
- Wiebers DO, Whisnant JP, Huston J 3rd, Meissner I, Brown RD Jr, Piepgras DG, Forbes GS, Thielen K, Nichols D, O’Fallon WM, Peacock J, Jaeger L, Kassell NF, et al., and International Study of Unruptured Intracranial Aneurysms Investigators. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet. 2003; 362:103–10. 10.1016/s0140-6736(03)13860-3 - DOI - PubMed
-
- Greving JP, Wermer MJ, Brown RD Jr, Morita A, Juvela S, Yonekura M, Ishibashi T, Torner JC, Nakayama T, Rinkel GJ, Algra A. Development of the PHASES score for prediction of risk of rupture of intracranial aneurysms: a pooled analysis of six prospective cohort studies. Lancet Neurol. 2014; 13:59–66. 10.1016/S1474-4422(13)70263-1 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
