

Genetic and immunologic findings in children with recurrent aphthous stomatitis with systemic inflammation
- PMID: 33971891
- PMCID: PMC8111718
- DOI: 10.1186/s12969-021-00552-y
Genetic and immunologic findings in children with recurrent aphthous stomatitis with systemic inflammation
Abstract
Background: Recurrent aphthous stomatitis with systemic signs of inflammation can be encountered in inflammatory bowel disease, Behçet's disease (BD), Systemic Lupus Erythematosus (SLE). In addition, it has been proposed that cases with very early onset in childhood can be underpinned by rare monogenic defects of immunity, which may require targeted treatments. Thus, subjects with early onset recurrent aphthous stomatitis receiving a clinical diagnosis of BD-like or SLE-like disease may deserve a further diagnostic workout, including immunologic and genetic investigations.
Objective: To investigate how an immunologic, genetic and transcriptomics assessment of interferon inflammation may improve diagnosis and care in children with recurrent aphthous stomatitis with systemic inflammation.
Methods: Subjects referred to the pediatric rheumatologist for recurrent aphthous stomatitis associated with signs of systemic inflammation from January 2015 to January 2020 were enrolled in the study and underwent analysis of peripheral lymphocyte subsets, sequencing of a 17-genes panel and measure of interferon score.
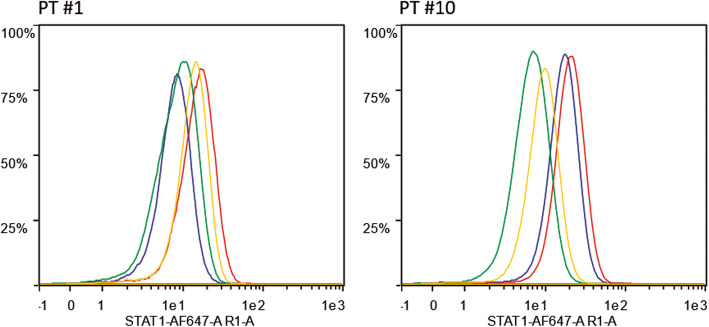
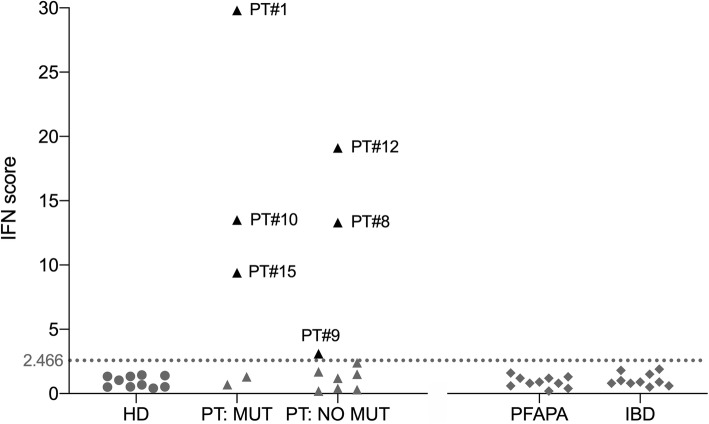
Results: We enrolled 15 subjects (12 females, median age at disease onset 4 years). The clinical diagnosis was BD in 8, incomplete BD in 5, BD/SLE overlap in 1, SLE in 1. Pathogenic genetic variants were detected in 3 patients, respectively 2 STAT1 gain of function variants in two patients classified as BD/SLE overlap and SLE, and 1 TNFAIP3 mutation (A20 haploinsufficiency) in patients with BD. Moreover 2 likely pathogenic variants were identified in DNASE1L3 and PTPN22, both in patients with incomplete BD. Interferon score was high in the two patients with STAT1 GOF mutations, in the patient with TNFAIP3 mutation, and in 3 genetic-negative subjects. In two patients, the treatment was modified based on genetic results.
Conclusions: Although recurrent aphthous stomatitis associated with systemic inflammation may lead to a clinical diagnosis of BD or SLE, subjects with early disease onset in childhood deserve genetic investigation for rare monogenic disorders. A wider genetic panel may help disclosing the genetic background in the subset of children with increased interferon score, who tested negative in this study.
Keywords: A20 haploinsufficiency; Behçet’s disease; Interferon signature; Recurrent aphthous stomatitis; STAT1 mutation; Systemic Lupus Erythematosus.
Conflict of interest statement
None of the Authors has any conflict of interests regarding the matters treated in the manuscript.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
