

Radiologic findings that aid in the reduction of misdiagnoses of Langerhans cell histiocytosis of the bone: a retrospective study
- PMID: 33971894
- PMCID: PMC8112044
- DOI: 10.1186/s12957-021-02261-y
Radiologic findings that aid in the reduction of misdiagnoses of Langerhans cell histiocytosis of the bone: a retrospective study
Abstract
Background: This study aimed to identify the characteristic radiological signs for the diagnosis of Langerhans cell histiocytosis (LCH) of the bone.
Methods: We retrospectively studied 82 cases of LCH with bone lesions confirmed by pathology. Clinical and radiological features of the patients were analyzed.
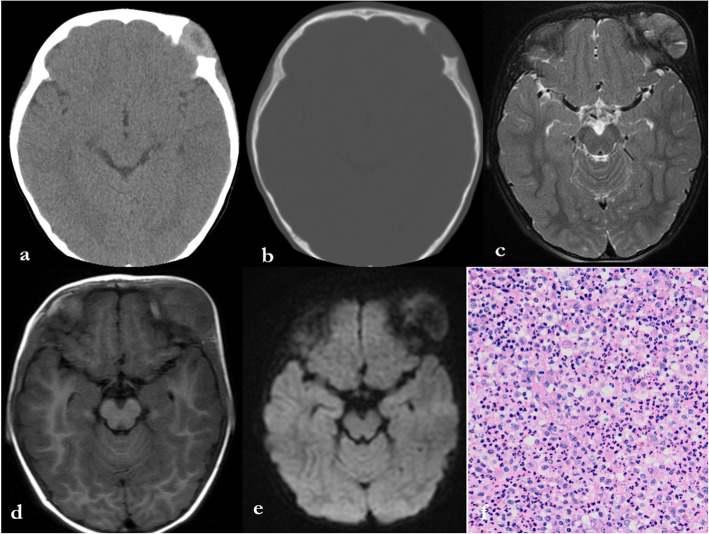
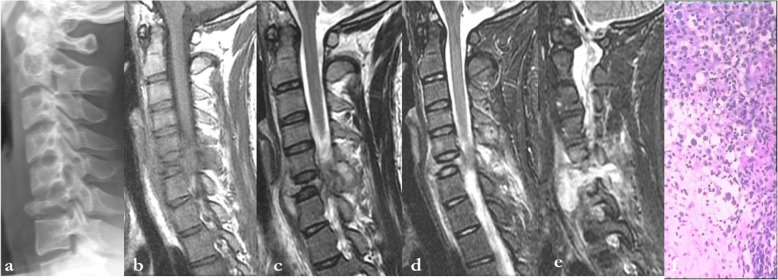
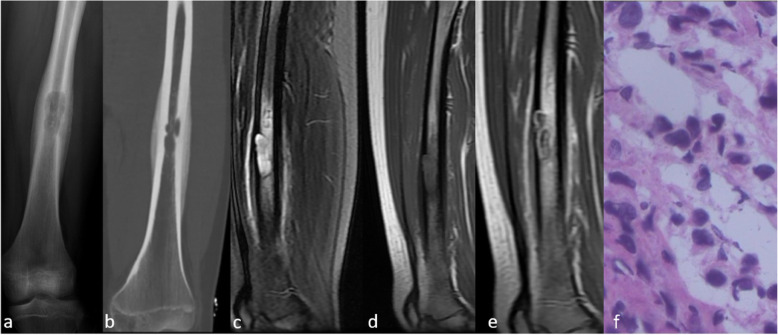
Results: A total of 64 and 18 patients had single and multiple bone lesions, respectively. With regard to LCH with single bone lesions, 37.5% (24/64) of lesions were located in the skull and presented as bone destruction with or without soft tissue mass. The correct diagnosis rate of these lesions was 60.0% (9/15) in children and adolescents, but was only 22.2% (2/9) in adults. A total of 26.5% (17/64) of the solitary lesions were found in the spine. Of these, 88.2% (15/17) were located in the vertebral body and appeared to have different degrees of collapse, and 66.7% (10/15) of these lesions were correctly diagnosed. Of the unifocal lesions, 21.8% (14/64) were located in other flat and irregular bones and manifested as osteolysis. Only 21.4% (3/14) of these cases were correctly diagnosed. In total, 14.1% (9/64) of the isolated bone LCH lesions were located in the long bones. Of these, 77.8% (7/9) were located in the diaphysis and presented as central bone destruction with or without fusiform periosteal reaction and extensive peripheral edema, of which 42.9% (3/7) were correctly diagnosed before surgery or biopsy. With regard to LCH with multiple bony destructive lesions, 71.4% (10/14) of cases in children and adolescents were correctly diagnosed; however, all four cases among adults were misdiagnosed.
Conclusion: In all age groups, isolated diaphyseal destruction of the long bone with fusiform periosteal reaction and extensive peripheral edema, vertebra plana of the spine, and bevelled edge of skull defects accompanied by soft tissue masses strongly suggest LCH diagnosis. Moreover, the multiple bone osteolytic destruction in children and adolescents strongly suggests LCH diagnosis. Familiarity with these typical radiological signs of LCH is necessary to decrease misdiagnoses.
Keywords: Bone lesion; Diagnostic imaging; Differential; Langerhans cell histiocytosis; Radiology.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Langerhans cell histiocytosis of spine: a comparative study of clinical, imaging features, and diagnosis in children, adolescents, and adults.Spine J. 2013 Sep;13(9):1108-17. doi: 10.1016/j.spinee.2013.03.013. Epub 2013 Apr 18. Spine J. 2013. PMID: 23602327
-
Ultrasonographic analysis of Langerhans cell histiocytosis in children: a report of 55 cases.J Int Med Res. 2022 Sep;50(9):3000605221126378. doi: 10.1177/03000605221126378. J Int Med Res. 2022. PMID: 36168708 Free PMC article.
-
MRI and clinical features of Langerhans cell histiocytosis (LCH) in the pelvis and extremities: can LCH really look like anything?Skeletal Radiol. 2016 May;45(5):607-13. doi: 10.1007/s00256-016-2330-x. Epub 2016 Jan 22. Skeletal Radiol. 2016. PMID: 26802000
-
Langerhans' cell histiocytosis: pathology, imaging and treatment of skeletal involvement.Pediatr Radiol. 2005 Feb;35(2):103-15. doi: 10.1007/s00247-004-1262-0. Epub 2004 Jul 28. Pediatr Radiol. 2005. PMID: 15289942 Review.
-
Oral manifestations of Langerhans cell histiocytosis with unusual histomorphologic features.Ann Diagn Pathol. 2020 Aug;47:151536. doi: 10.1016/j.anndiagpath.2020.151536. Epub 2020 May 21. Ann Diagn Pathol. 2020. PMID: 32454442 Review.
Cited by
-
Adult-onset Langerhans cell histiocytosis with multisystem involvement: A rare case report.Radiol Case Rep. 2024 Dec 11;20(3):1289-1293. doi: 10.1016/j.radcr.2024.11.069. eCollection 2025 Mar. Radiol Case Rep. 2024. PMID: 39758329 Free PMC article.
-
Adult Langerhans Cell Histiocytosis and the Skeleton.J Clin Med. 2022 Feb 9;11(4):909. doi: 10.3390/jcm11040909. J Clin Med. 2022. PMID: 35207181 Free PMC article. Review.
-
Imaging features of pediatric meningiomas: emphasis on unusual locations.Childs Nerv Syst. 2024 Dec;40(12):3933-3942. doi: 10.1007/s00381-024-06525-2. Epub 2024 Jul 10. Childs Nerv Syst. 2024. PMID: 38985317
-
Langerhans cell histiocytosis of the jaw: clinical analysis of 68 cases.Orphanet J Rare Dis. 2025 Apr 21;20(1):191. doi: 10.1186/s13023-025-03680-w. Orphanet J Rare Dis. 2025. PMID: 40259405 Free PMC article.
References
-
- Emile J, Abla O, Fraitag S, Horne A, Haroche J, Donadieu J, Requena-Caballero L, Jordan MB, Abdel-Wahab O, Allen CE, Charlotte F, Diamond EL, Egeler RM, Fischer A, Herrera JG, Henter JI, Janku F, Merad M, Picarsic J, Rodriguez-Galindo C, Rollins BJ, Tazi A, Vassallo R, Weiss LM, Histiocyte Society Revised classification of histiocytoses and neoplasms of the macrophage-dendritic cell lineages. Blood. 2016;127(22):2672–2681. doi: 10.1182/blood-2016-01-690636. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
