

Effects of a robot-aided somatosensory training on proprioception and motor function in stroke survivors
- PMID: 33971912
- PMCID: PMC8112068
- DOI: 10.1186/s12984-021-00871-x
Effects of a robot-aided somatosensory training on proprioception and motor function in stroke survivors
Erratum in
-
Correction to: Effects of a robot-aided somatosensory training on proprioception and motor function in stroke survivors.J Neuroeng Rehabil. 2022 Jul 18;19(1):74. doi: 10.1186/s12984-022-01057-9. J Neuroeng Rehabil. 2022. PMID: 35850764 Free PMC article. No abstract available.
Abstract
Background: Proprioceptive deficits after stroke are associated with poor upper limb function, slower motor recovery, and decreased self-care ability. Improving proprioception should enhance motor control in stroke survivors, but current evidence is inconclusive. Thus, this study examined whether a robot-aided somatosensory-based training requiring increasingly accurate active wrist movements improves proprioceptive acuity as well as motor performance in chronic stroke.
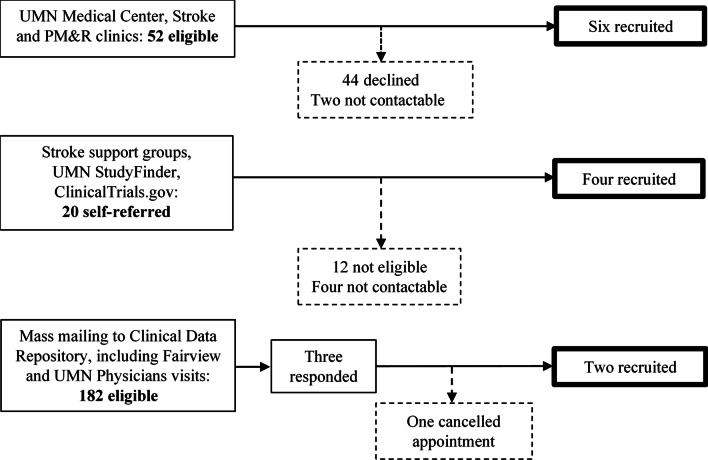
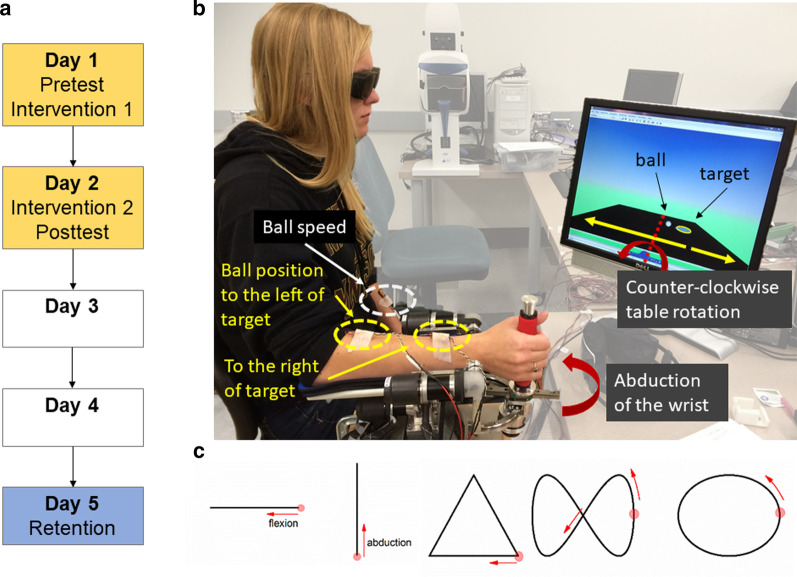
Methods: Twelve adults with chronic stroke completed a 2-day training (age range: 42-74 years; median time-after-stroke: 12 months; median Fugl-Meyer UE: 65). Retention was assessed at Day 5. Grasping the handle of a wrist-robotic exoskeleton, participants trained to roll a virtual ball to a target through continuous wrist adduction/abduction movements. During training vision was occluded, but participants received real-time, vibro-tactile feedback on their forearm about ball position and speed. Primary outcome was the just-noticeable-difference (JND) wrist position sense threshold as a measure of proprioceptive acuity. Secondary outcomes were spatial error in an untrained wrist tracing task and somatosensory-evoked potentials (SEP) as a neural correlate of proprioceptive function. Ten neurologically-intact adults were recruited to serve as non-stroke controls for matched age, gender and hand dominance (age range: 44 to 79 years; 6 women, 4 men).
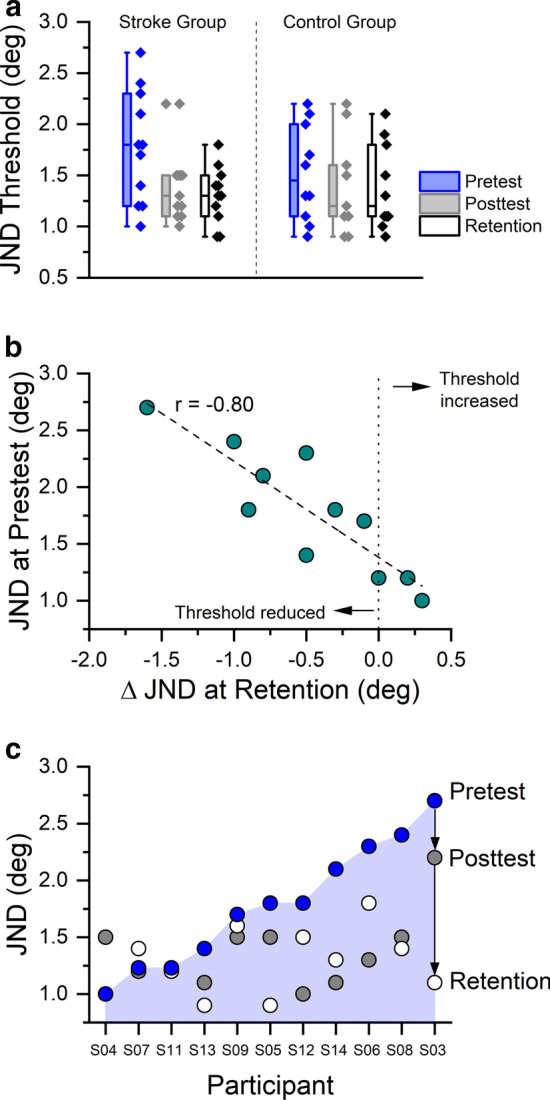
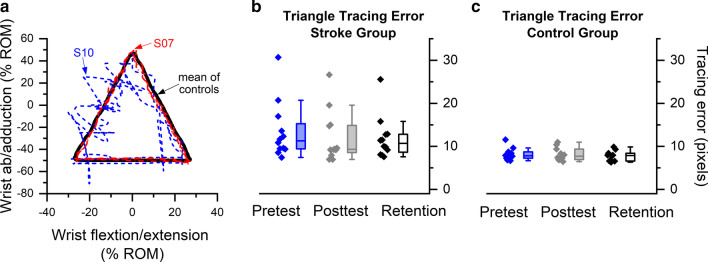
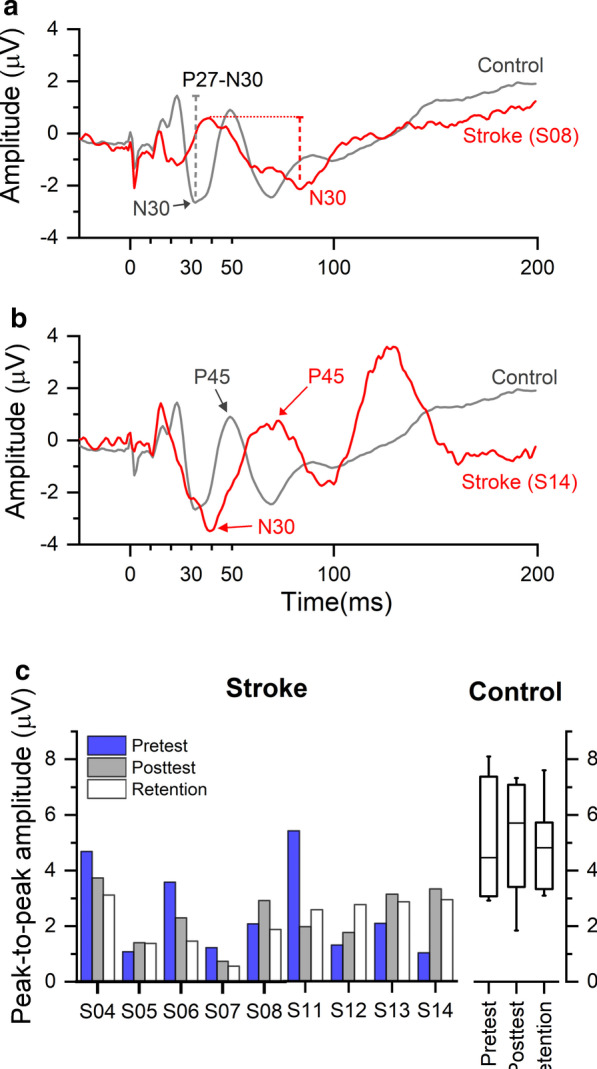
Results: Participants significantly reduced JND thresholds at posttest and retention (Stroke group: pretest: mean: 1.77° [SD: 0.54°] to posttest mean: 1.38° [0.34°]; Control group: 1.50° [0.46°] to posttest mean: 1.45° [SD: 0.54°]; F[2,37] = 4.54, p = 0.017, ηp2 = 0.20) in both groups. A higher pretest JND threshold was associated with a higher threshold reduction at posttest and retention (r = - 0.86, - 0.90, p ≤ 0.001) among the stroke participants. Error in the untrained tracing task was reduced by 22 % at posttest, yielding an effect size of w = 0.13. Stroke participants exhibited significantly reduced P27-N30 peak-to-peak SEP amplitude at pretest (U = 11, p = 0.03) compared to the non-stroke group. SEP measures did not change systematically with training.
Conclusions: This study provides proof-of-concept that non-visual, proprioceptive training can induce fast, measurable improvements in proprioceptive function in chronic stroke survivors. There is encouraging but inconclusive evidence that such somatosensory learning transfers to untrained motor tasks. Trial registration Clinicaltrials.gov; Registration ID: NCT02565407; Date of registration: 01/10/2015; URL: https://clinicaltrials.gov/ct2/show/NCT02565407 .
Keywords: Cerebrovascular disease/stroke; Human; Rehabilitation; Somatosensation; Upper limb.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
