

Validating online approaches for rare disease research using latent class mixture modeling
- PMID: 33971926
- PMCID: PMC8108361
- DOI: 10.1186/s13023-021-01827-z
Validating online approaches for rare disease research using latent class mixture modeling
Abstract
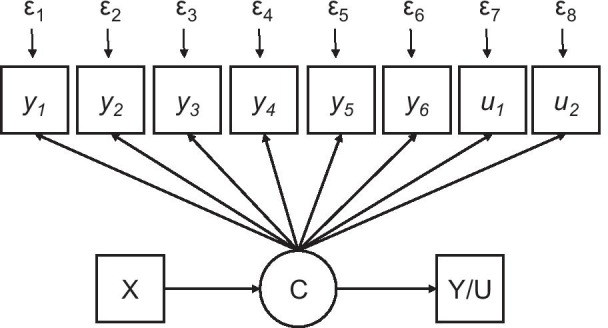
Background: Rare disease patients are geographically dispersed, posing challenges to research. Some researchers have partnered with patient organizations and used web-based approaches to overcome geographic recruitment barriers. Critics of such methods claim that samples are homogenous and do not represent the broader patient population-as patients recruited from patient organizations are thought to have high levels of needs. We applied latent class mixture modeling (LCMM) to define patient clusters based on underlying characteristics. We used previously collected data from a cohort of patients with congenital hypogonadotropic hypogonadism who were recruited online in collaboration with a patient organization. Patient demographics, clinical information, Revised Illness Perception Questionnaire (IPQ-R) scores and Zung self-rating depression Scale (SDS) were used as variables for LCMM analysis. Specifically, we aimed to test the classic critique that patients recruited online in collaboration with a patient organization are a homogenous group with high needs. We hypothesized that distinct classes (clinical profiles) of patients could be identified-thereby demonstrating the validity of online recruitment and supporting transferability of findings.
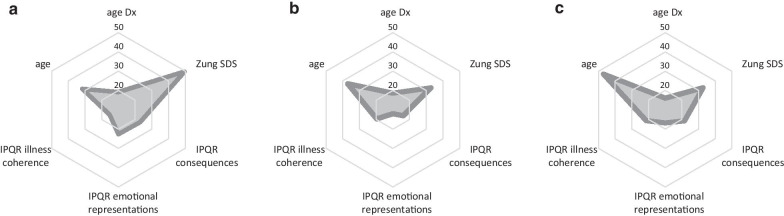
Results: In total, 154 patients with CHH were included. The LCMM analysis identified three distinct subgroups (Class I: n = 84 [54.5%], Class II: n = 41 [26.6%], Class III: n = 29 [18.8%]) that differed significantly in terms of age, education, disease consequences, emotional consequences, illness coherence and depression symptoms (all p < 0.001) as well as age at diagnosis (p = 0.045). Classes depict a continuum of psychosocial impact ranging from severe to relatively modest. Additional analyses revealed later diagnosis (Class I: 19.2 ± 6.7 years [95% CI 17.8-20.7]) is significantly associated with worse psychological adaptation and coping as assessed by disease consequences, emotional responses, making sense of one's illness and SDS depressive symptoms (all p < 0.001).
Conclusions: We identify three distinct classes of patients who were recruited online in collaboration with a patient organization. Findings refute prior critiques of patient partnership and web-based recruitment for rare disease research. This is the first empirical data suggesting negative psychosocial sequelae of later diagnosis ("diagnostic odyssey") often observed in CHH.
Keywords: Community based participatory research; Diagnostic odyssey; Hypogonadotropic hypogonadism; Kallmann syndrome; Patient organization; Rare disease.
Conflict of interest statement
The authors have no financial or non-financial competing interests to declare.
Figures
References
-
- Kempf L, Goldsmith JC, Temple R. Challenges of developing and conducting clinical trials in rare disorders. Am J Med Genet A. 2018;176:773–783. - PubMed
-
- EURORDIS: The voice of 12,000 patients: Experiences and expectations of rare disease patients on diagnosis and care in Europe. In Book The voice of 12,000 patients: Experiences and expectations of rare disease patients on diagnosis and care in Europe (Editor ed.^eds.). City; 2009.
-
- Fox S. Peer-to-Peer Healthcare. Washington: Pew Internet; 2011.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
