

Accessing routinely collected health data to improve clinical trials: recent experience of access
- PMID: 33971933
- PMCID: PMC8108438
- DOI: 10.1186/s13063-021-05295-5
Accessing routinely collected health data to improve clinical trials: recent experience of access
Abstract
Background: Routinely collected electronic health records (EHRs) have the potential to enhance randomised controlled trials (RCTs) by facilitating recruitment and follow-up. Despite this, current EHR use is minimal in UK RCTs, in part due to ongoing concerns about the utility (reliability, completeness, accuracy) and accessibility of the data. The aim of this manuscript is to document the process, timelines and challenges of the application process to help improve the service both for the applicants and data holders.
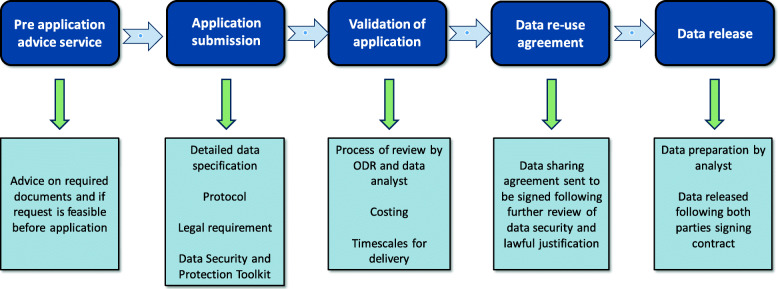
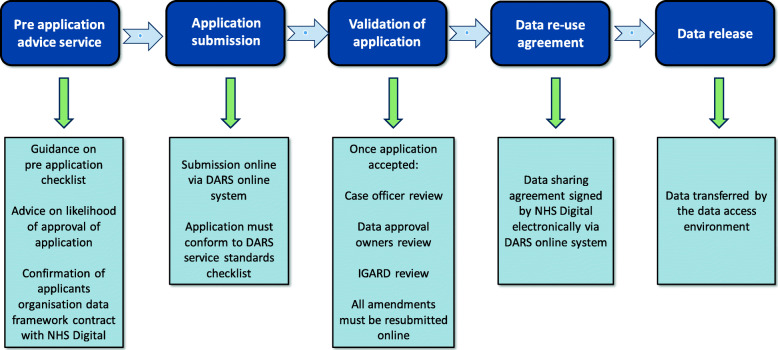
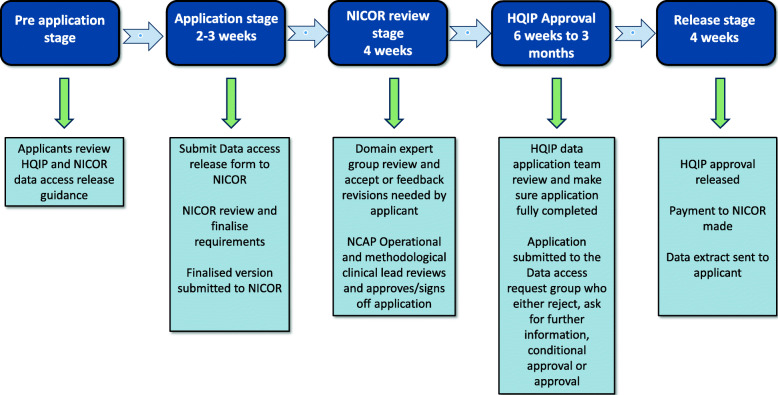
Methods: This is a qualitative paper providing a descriptive narrative from one UK clinical trials unit (MRC CTU at UCL) on the experience of two trial teams' application process to access data from three large English national datasets: National Cancer Registration and Analysis Service (NCRAS), National Institute for Cardiovascular Outcomes Research (NICOR) and NHS Digital to establish themes for discussion. The underpinning reason for applying for the data was to compare EHRs with data collected through case report forms in two RCTs, Add-Aspirin (ISRCTN 74358648) and PATCH (ISRCTN 70406718).
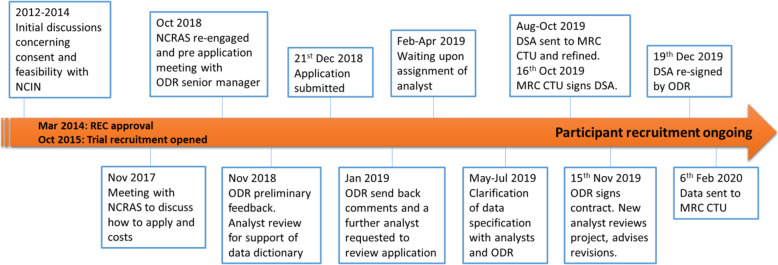
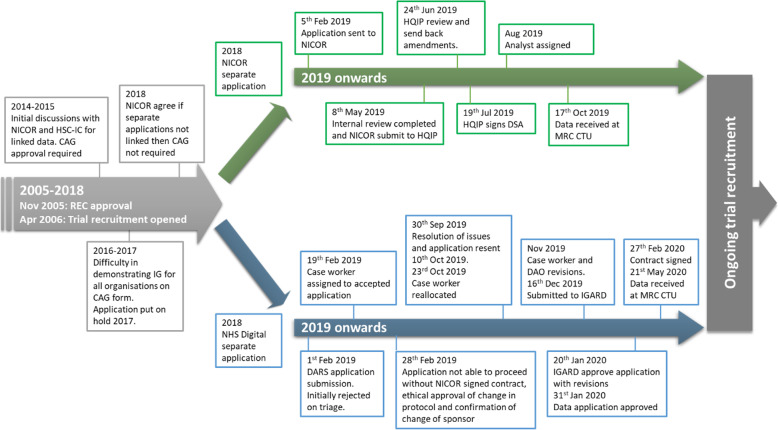
Results: The Add-Aspirin trial, which had a pre-planned embedded sub-study to assess EHR, received data from NCRAS 13 months after the first application. In the PATCH trial, the decision to request data was made whilst the trial was recruiting. The study received data after 8 months from NICOR and 15 months for NHS Digital following final application submission. This concluded in May 2020. Prior to application submission, significant time and effort was needed particularly in relation to the PATCH trial where negotiations over consent and data linkage took many years.
Conclusions: Our experience demonstrates that data access can be a prolonged and complex process. This is compounded if multiple data sources are required for the same project. This needs to be factored in when planning to use EHR within RCTs and is best considered prior to conception of the trial. Data holders and researchers are endeavouring to simplify and streamline the application process so that the potential of EHR can be realised for clinical trials.
Keywords: Clinical trials; Data accessibility; Electronic health records; Routinely collected data.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- Lagerqvist B, Fröbert O, Olivecrona GK, Gudnason T, Maeng M, Alström P, Andersson J, Calais F, Carlsson J, Collste O, Götberg M, Hårdhammar P, Ioanes D, Kallryd A, Linder R, Lundin A, Odenstedt J, Omerovic E, Puskar V, Tödt T, Zelleroth E, Östlund O, James SK. Outcomes 1 year after thrombus aspiration for myocardial infarction. New Engl J Med. 2014;371(12):1111–1120. doi: 10.1056/NEJMoa1405707. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
