

Gambogic acid protects LPS-induced apoptosis and inflammation in a cell model of neonatal pneumonia through the regulation of TrkA/Akt signaling pathway
- PMID: 33971977
- PMCID: PMC8112032
- DOI: 10.1186/s40360-021-00496-9
Gambogic acid protects LPS-induced apoptosis and inflammation in a cell model of neonatal pneumonia through the regulation of TrkA/Akt signaling pathway
Abstract
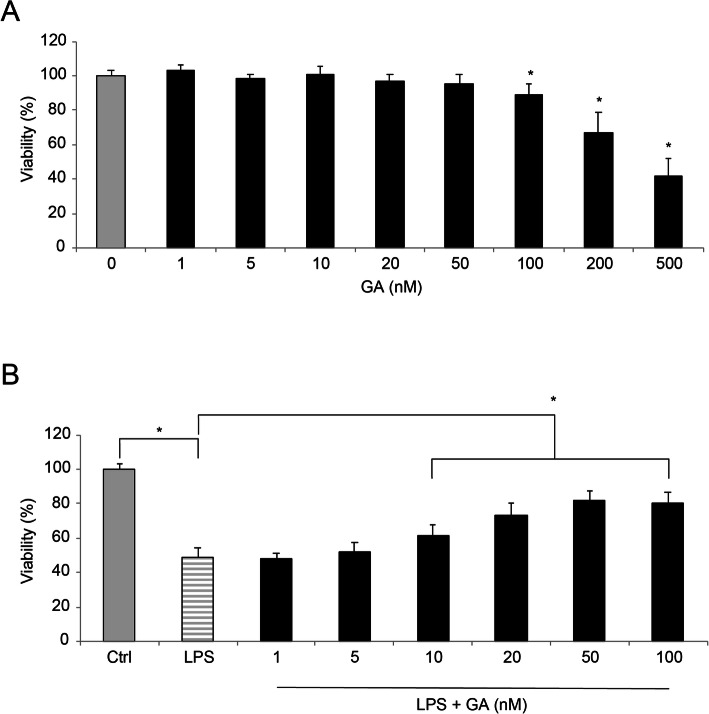
Objective: In this work, we investigated the effects of gambogic acid (GA) on lipopolysaccharide (LPS)-induced apoptosis and inflammation in a cell model of neonatal pneumonia.
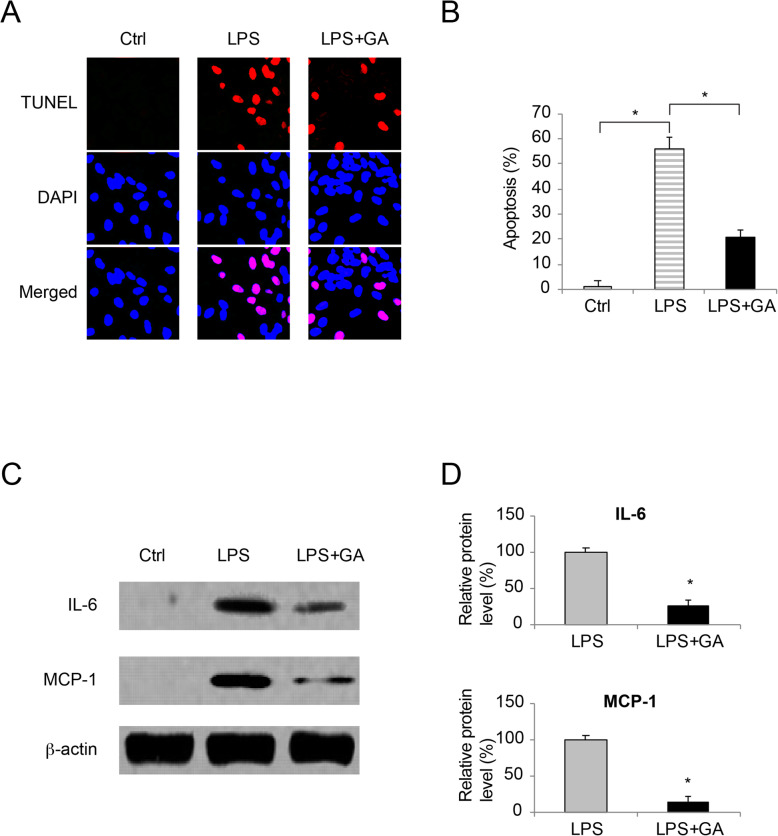
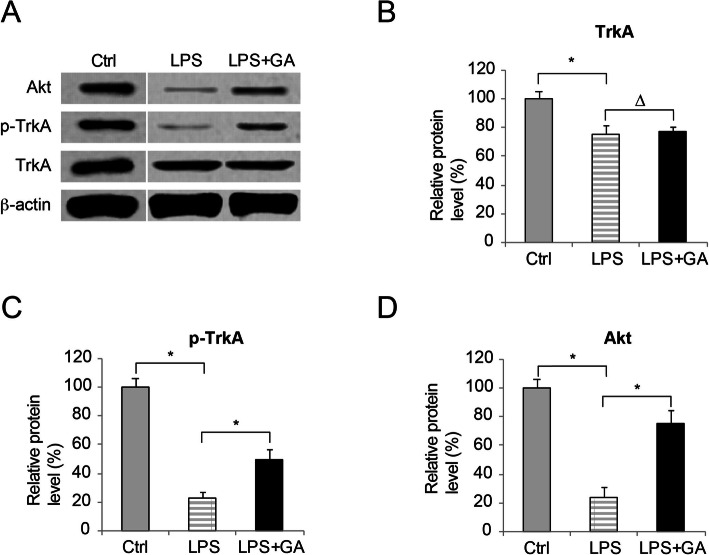
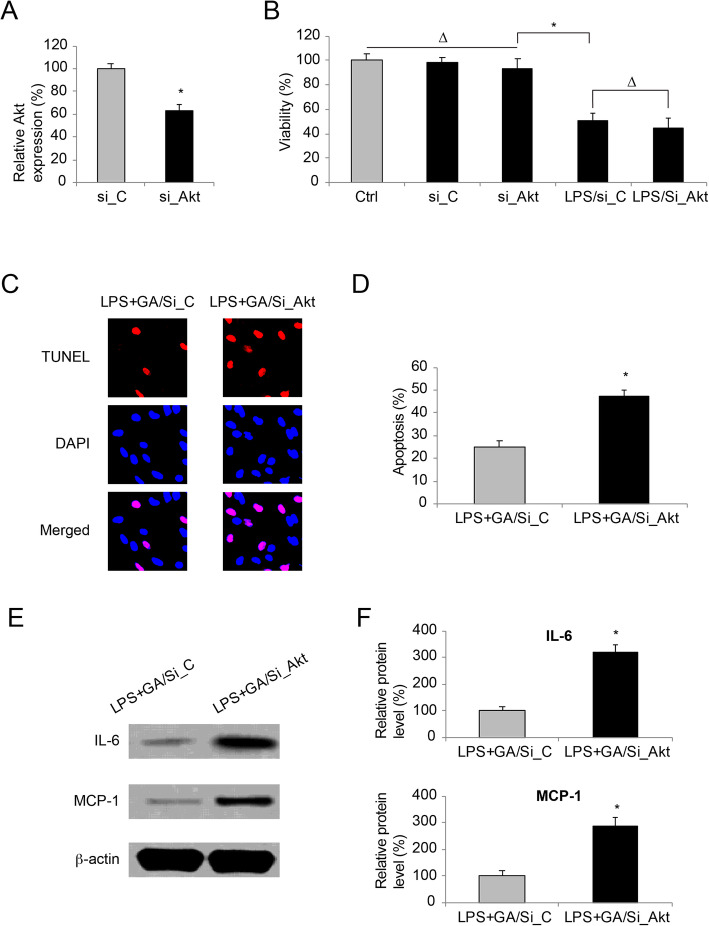
Method: Human WI-38 cells were maintained in vitro and incubated with various concentrations of GA to examine WI-38 survival. GA-preincubated WI-38 cells were then treated with LPS to investigate the protective effects of GA on LPS-induced death, apoptosis and inflammation. Western blot assay was utilized to analyze the effect of GA on tropomyosin receptor kinase A (TrkA) signaling pathway in LPS-treated WI-38 cells. In addition, human AKT serine/threonine kinase 1 (Akt) gene was knocked down in WI-38 cells to further investigate the associated genetic mechanisms of GA in protecting LPS-induced inflammation and apoptosis.
Results: Pre-incubating WI-38 cells with low and medium concentrations GA protected LPS-induced cell death, apoptosis and inflammatory protein productions of IL-6 and MCP-1. Using western blot assay, it was demonstrated that GA promoted TrkA phosphorylation and Akt activation in LPS-treated WI-38 cells. Knocking down Akt gene in WI-38 cells showed that GA-associated protections against LPS-induced apoptosis and inflammation were significantly reduced.
Conclusions: GA protected LPS-induced apoptosis and inflammation, possibly through the activations of TrkA and Akt signaling pathway. This work may broaden our understanding on the molecular mechanisms of human neonatal pneumonia.
Keywords: Neonatal pneumonia; apoptosis; gambogic acid; inflammation; lipopolysaccharide.
Conflict of interest statement
None
Figures
Similar articles
-
Phentolamine Protects against Apoptosis and Inflammation in a Neonatal Pneumonia Cell Model Induced by LPS by Regulating the TrkA/Akt Signaling Pathways.Discov Med. 2024 Mar;36(182):581-590. doi: 10.24976/Discov.Med.202436182.54. Discov Med. 2024. PMID: 38531798
-
Gambogic acid alleviates inflammation and apoptosis and protects the blood-milk barrier in mastitis induced by LPS.Int Immunopharmacol. 2020 Sep;86:106697. doi: 10.1016/j.intimp.2020.106697. Epub 2020 Jun 22. Int Immunopharmacol. 2020. PMID: 32585608
-
Curcumin alleviates LPS-induced WI-38 cell inflammation injury by regulating PTGS2 expression.Hereditas. 2025 May 16;162(1):81. doi: 10.1186/s41065-025-00441-4. Hereditas. 2025. PMID: 40380246 Free PMC article.
-
Coniferyl aldehyde alleviates LPS-induced WI-38 cell apoptosis and inflammation injury via JAK2-STAT1 pathway in acute pneumonia.Allergol Immunopathol (Madr). 2021 Sep 1;49(5):72-77. doi: 10.15586/aei.v49i5.464. eCollection 2021. Allergol Immunopathol (Madr). 2021. PMID: 34476925
-
Long noncoding RNA SNHG16 targets miR-146a-5p/CCL5 to regulate LPS-induced WI-38 cell apoptosis and inflammation in acute pneumonia.Life Sci. 2019 Jul 1;228:189-197. doi: 10.1016/j.lfs.2019.05.008. Epub 2019 May 7. Life Sci. 2019. PMID: 31071307 Review.
Cited by
-
Gambogic acid targets HSP90 to alleviate DSS-induced colitis via inhibiting the necroptosis of intestinal epithelial cells.Front Pharmacol. 2025 May 19;16:1586705. doi: 10.3389/fphar.2025.1586705. eCollection 2025. Front Pharmacol. 2025. PMID: 40458801 Free PMC article.
-
Mechanisms of the effects of turpiniae folium extract on growth performance, immunity, antioxidant activity and intestinal barrier function in LPS-challenged broilers.Poult Sci. 2025 Apr;104(4):104903. doi: 10.1016/j.psj.2025.104903. Epub 2025 Feb 17. Poult Sci. 2025. PMID: 39985896 Free PMC article.
-
Post Natal Microbial and Metabolite Transmission: The Path from Mother to Infant.Nutrients. 2024 Jun 22;16(13):1990. doi: 10.3390/nu16131990. Nutrients. 2024. PMID: 38999737 Free PMC article.
-
Rutin-chitooligosaccharide complex: Comprehensive evaluation of its anti-inflammatory and analgesic properties in vitro and in vivo.Open Life Sci. 2025 Mar 6;20(1):20221021. doi: 10.1515/biol-2022-1021. eCollection 2025. Open Life Sci. 2025. PMID: 40059877 Free PMC article.
-
Targeting lncRNAs of colorectal cancers with natural products.Front Pharmacol. 2023 Jan 9;13:1050032. doi: 10.3389/fphar.2022.1050032. eCollection 2022. Front Pharmacol. 2023. PMID: 36699052 Free PMC article. Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
