

Placental Function and the Development of Fetal Overgrowth and Fetal Growth Restriction
- PMID: 33972064
- PMCID: PMC8117119
- DOI: 10.1016/j.ogc.2021.02.001
Placental Function and the Development of Fetal Overgrowth and Fetal Growth Restriction
Abstract
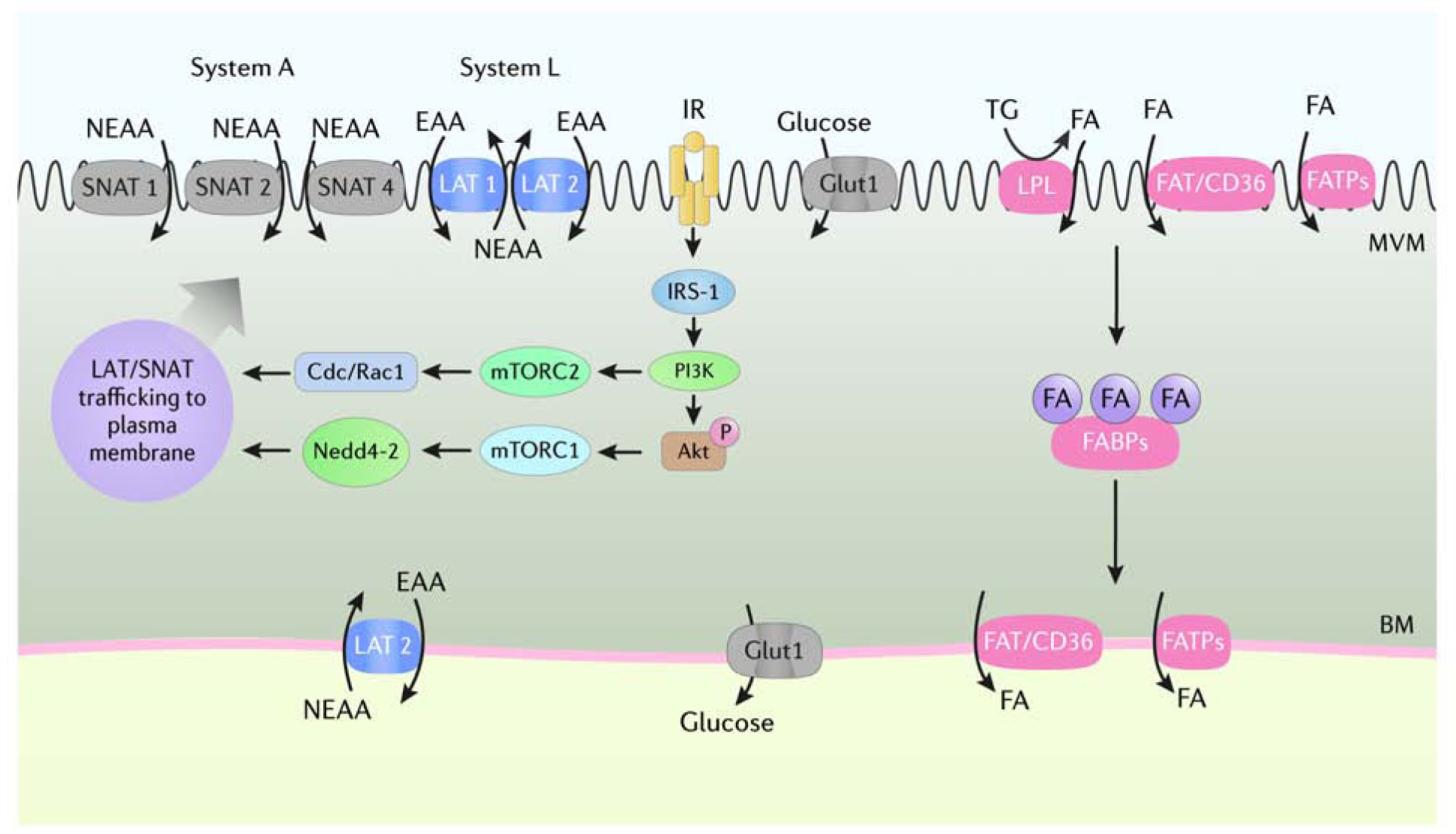
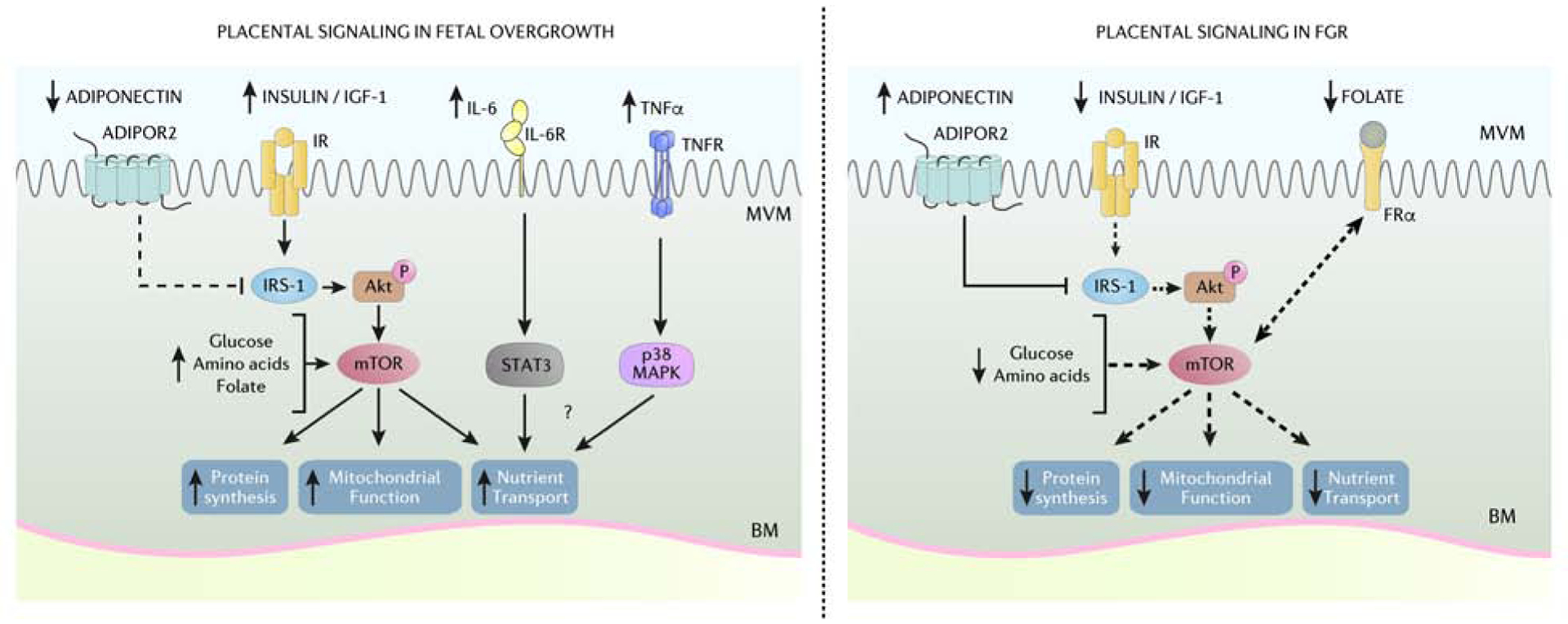
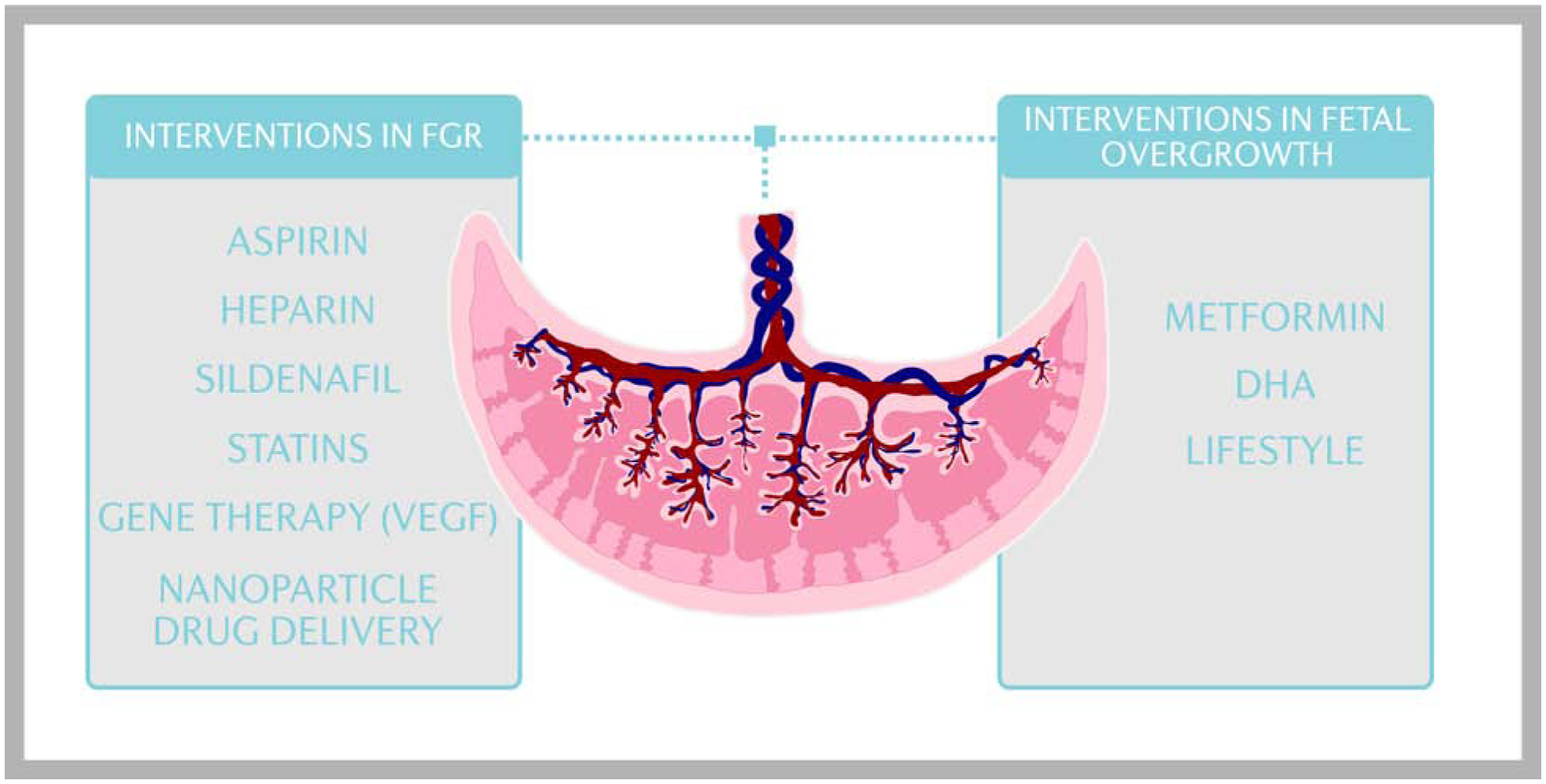
Placental regulation of fetal growth involves the integration of multiple signaling pathways that modulate an array of placental functions, including nutrient transport. As a result, the flux of oxygen and nutrients to the fetus is altered, leading to changes in placental and fetal growth. Placental insulin/insulinlike growth factor-1 and mechanistic target of rapamycin signaling and amino acid transport capacity are inhibited in fetal growth restriction and activated in fetal overgrowth, implicating these placental functions in driving fetal growth. With novel approaches to specifically target the placenta, clinical interventions to modulate placental function in high-risk pregnancies can be developed.
Keywords: Fetal development; Fetal growth restriction; Fetal overgrowth; Maternal-fetal exchange; Placental transport; Syncytiotrophoblast.
Copyright © 2021 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Catalano PM, Ehrenberg HM. The short- and long-term implications of maternal obesity on the mother and her offspring. BJOG. 2006;113(10):1126–1133. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
