

Case of cerebellar ataxia successfully treated by virtual reality-guided rehabilitation
- PMID: 33972306
- PMCID: PMC8112436
- DOI: 10.1136/bcr-2021-242287
Case of cerebellar ataxia successfully treated by virtual reality-guided rehabilitation
Abstract
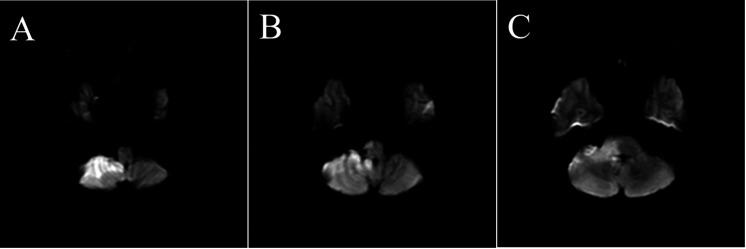
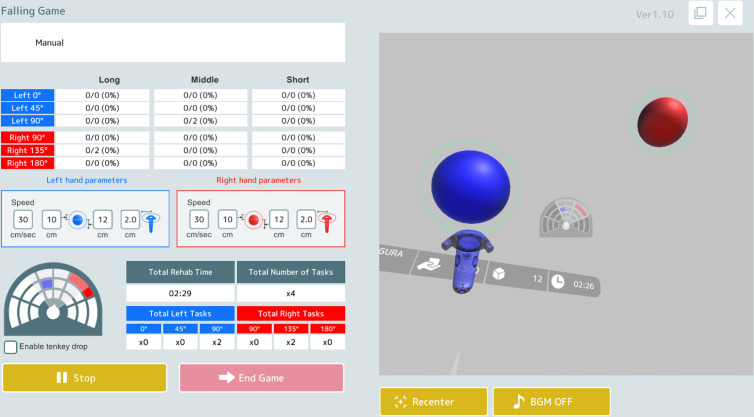
A male patient in his 40s was transferred to our hospital for rehabilitation of ataxia after right cerebellar and brainstem infarction. After 3 weeks of conventional physical therapy, his activities of daily life successfully improved with an increase in the functional impedance measure from 101 to 124. However, he still fell short of gaining a higher level of balance function, which was necessary for his job as a standup forklift driver. We introduced virtual reality-guided balance training. The training was performed for approximately 40 min on weekdays for 2 weeks. As a result, the Scale for the Assessment and Rating of Ataxia score decreased from 5 to 1, Functional Balance Scale score improved from 48 to 56, and Mini-Balance Evaluation Systems Test score increased from 20 to 28. The trunk sway disappeared clinically. He regained confidence and returned to work after an additional 2 weeks of physical therapy.
Keywords: brain stem / cerebellum; physiotherapy (rehabilitation); rehabilitation medicine; virtual rehabilitation.
© BMJ Publishing Group Limited 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: YM is an employee of mediVR, a company that holds several patents on VR-guided rehabilitation. KT, KO and HI have no conflicts of interest to declare.
Figures

References
-
- Carr JH, Shepherd RB. Neurological rehabilitation, 2nd edition. optimizing motor performance. In: Churchill Livingstone Elsevier, 2010: 217–34.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials