

Comprehensive pregnancy monitoring with a network of wireless, soft, and flexible sensors in high- and low-resource health settings
- PMID: 33972445
- PMCID: PMC8157941
- DOI: 10.1073/pnas.2100466118
Comprehensive pregnancy monitoring with a network of wireless, soft, and flexible sensors in high- and low-resource health settings
Abstract
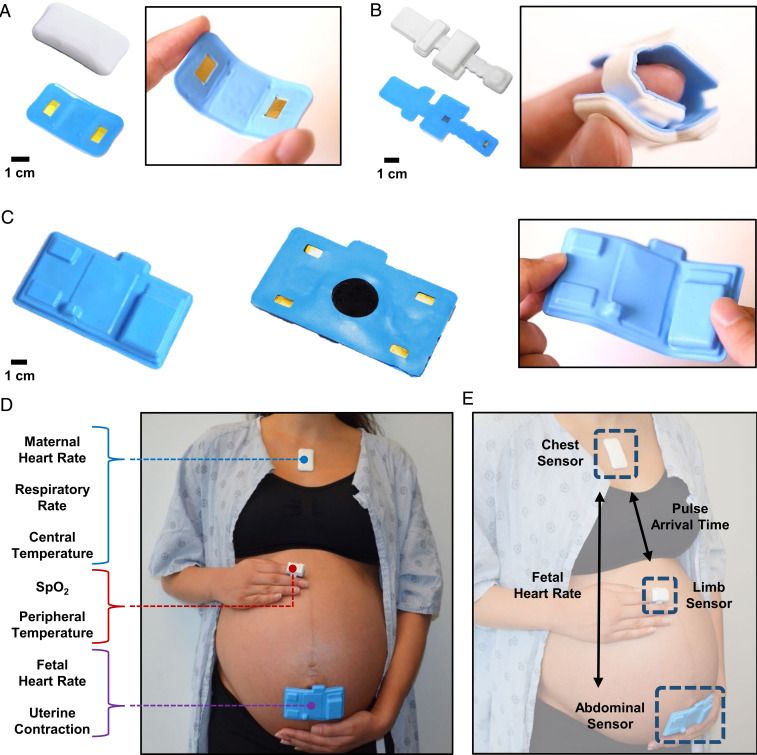
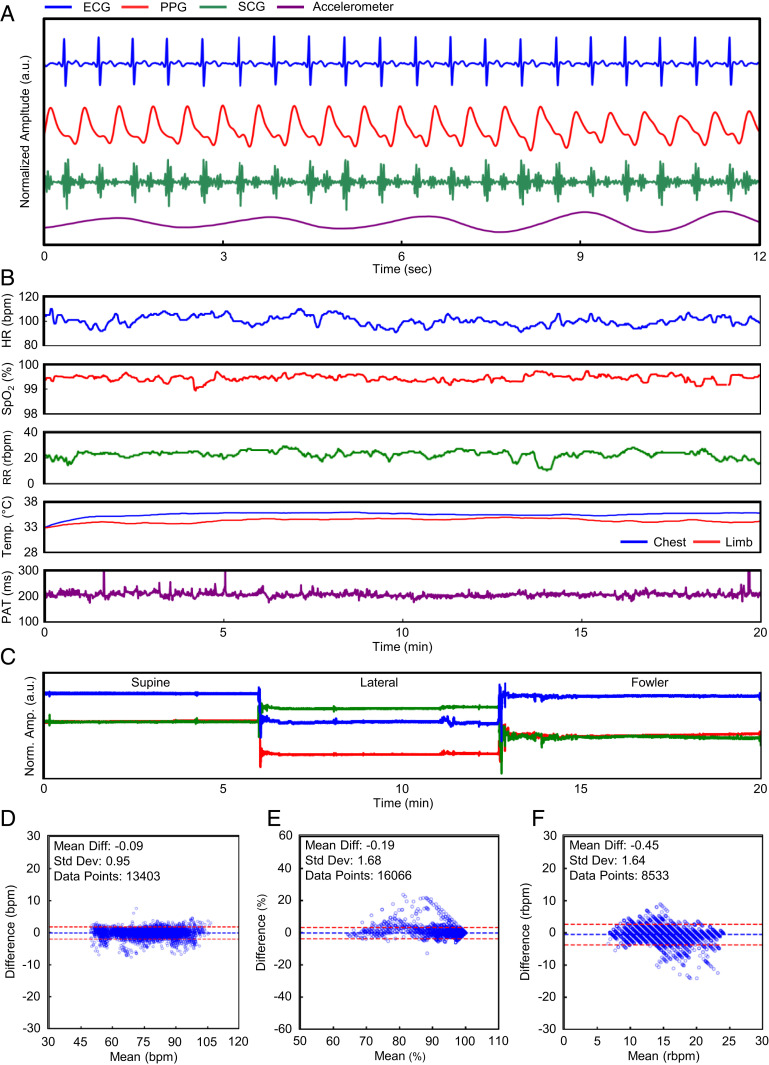
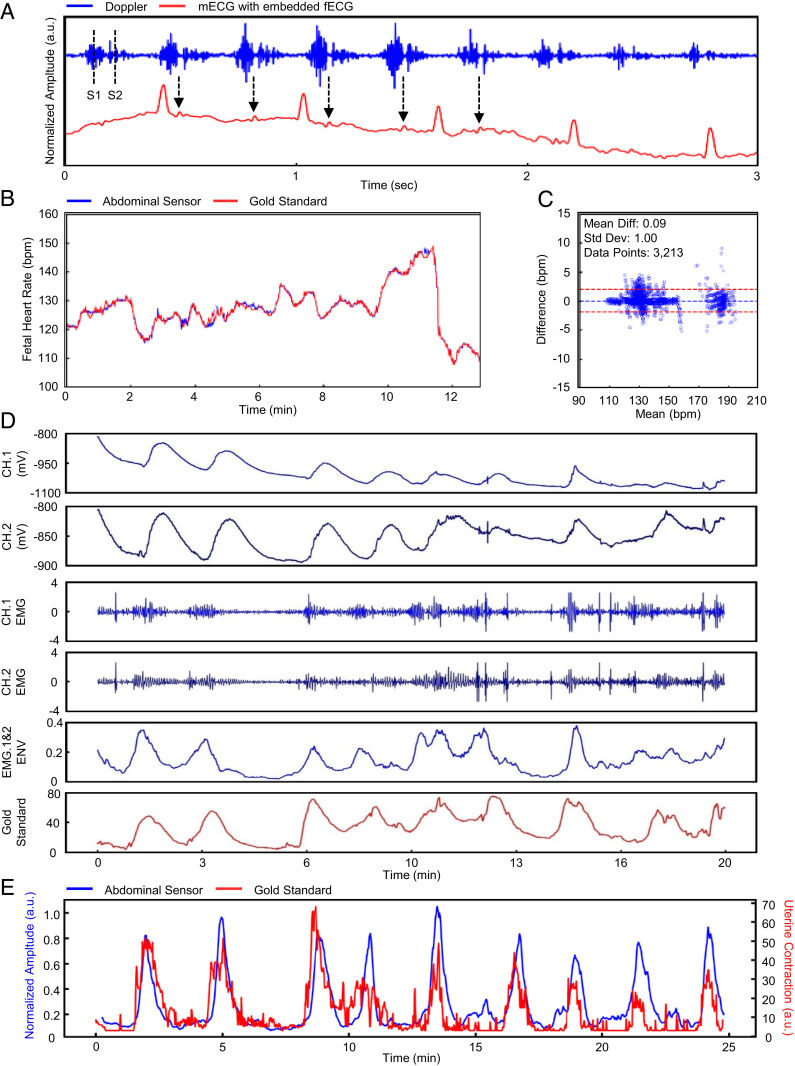
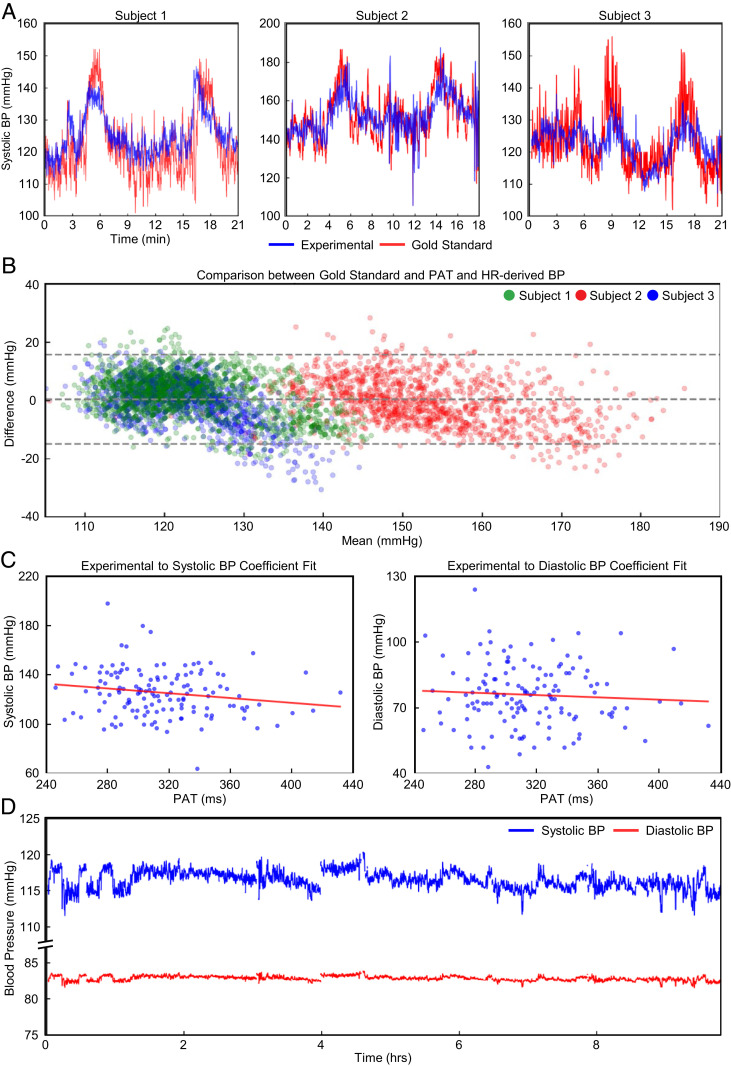
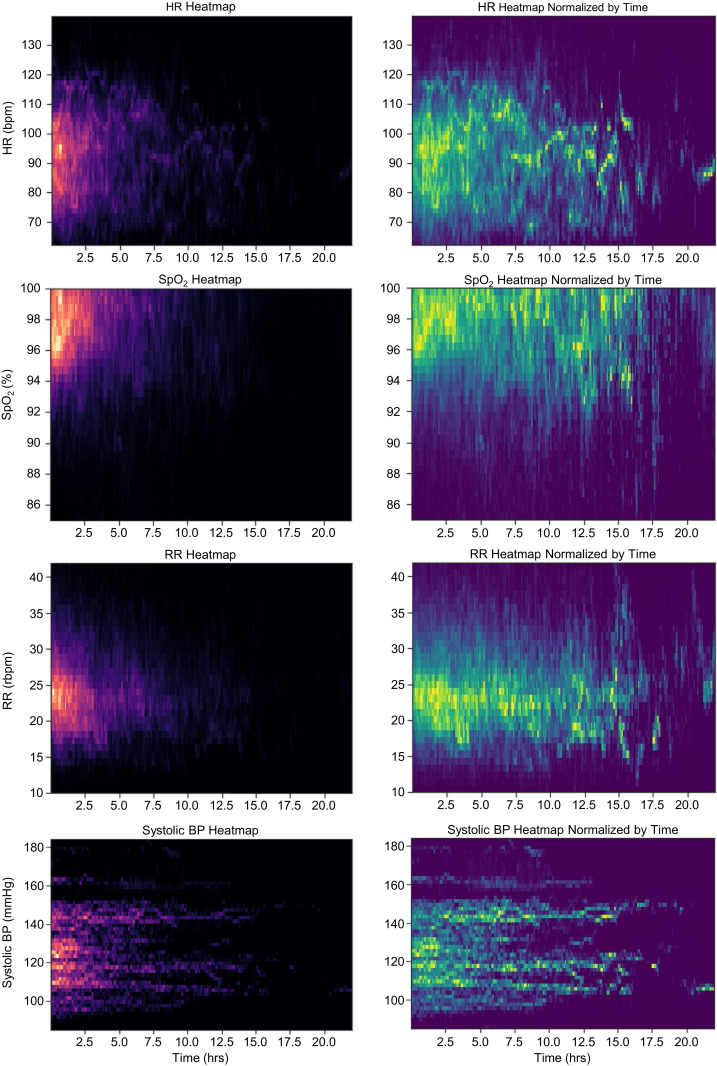
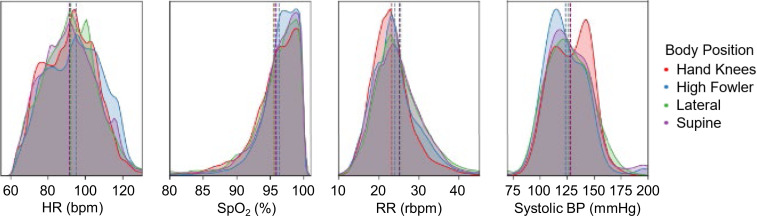
Vital signs monitoring is a fundamental component of ensuring the health and safety of women and newborns during pregnancy, labor, and childbirth. This monitoring is often the first step in early detection of pregnancy abnormalities, providing an opportunity for prompt, effective intervention to prevent maternal and neonatal morbidity and mortality. Contemporary pregnancy monitoring systems require numerous devices wired to large base units; at least five separate devices with distinct user interfaces are commonly used to detect uterine contractility, maternal blood oxygenation, temperature, heart rate, blood pressure, and fetal heart rate. Current monitoring technologies are expensive and complex with implementation challenges in low-resource settings where maternal morbidity and mortality is the greatest. We present an integrated monitoring platform leveraging advanced flexible electronics, wireless connectivity, and compatibility with a wide range of low-cost mobile devices. Three flexible, soft, and low-profile sensors offer comprehensive vital signs monitoring for both women and fetuses with time-synchronized operation, including advanced parameters such as continuous cuffless blood pressure, electrohysterography-derived uterine monitoring, and automated body position classification. Successful field trials of pregnant women between 25 and 41 wk of gestation in both high-resource settings (n = 91) and low-resource settings (n = 485) demonstrate the system's performance, usability, and safety.
Keywords: biosensors; pregnancy; vital signs.
Copyright © 2021 the Author(s). Published by PNAS.
Conflict of interest statement
Competing interest statement: Coauthors with a Sibel, Inc. affiliation are working with the Bill & Melinda Gates Foundation to deploy these technologies into low- and middle-income countries.
Figures
References
-
- Organization World Health, Trends in Maternal Mortality 2000 to 2017: Estimates by WHO, UNICEF, UNFPA (World Bank Group and the United Nations Population Division, 2019).
-
- Rochat R. W., Koonin L. M., Atrash H. K., Jewett J. F., Maternal mortality in the United States: Report from the maternal mortality collaborative. Obstet. Gynecol. 72, 91–97 (1988). - PubMed
-
- Kodio B., et al., Levels and causes of maternal mortality in Senegal. Trop. Med. Int. Health 7, 499–505 (2002). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
