

A Rare Case of Early Transformation of Gestational Trophoblastic Neoplasia Following Molar Pregnancy
- PMID: 33972495
- PMCID: PMC8126585
- DOI: 10.12659/AJCR.930789
A Rare Case of Early Transformation of Gestational Trophoblastic Neoplasia Following Molar Pregnancy
Abstract
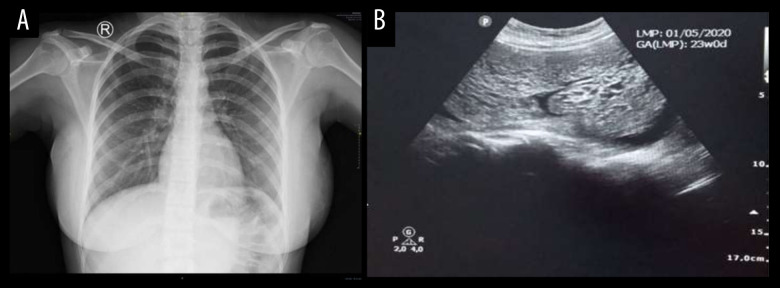
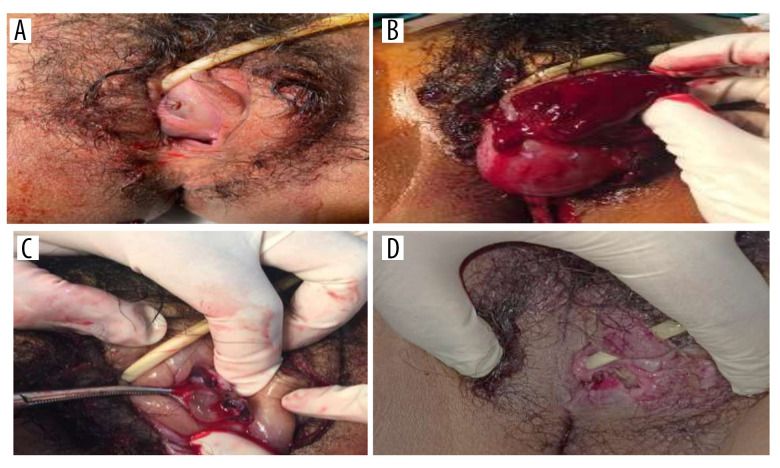
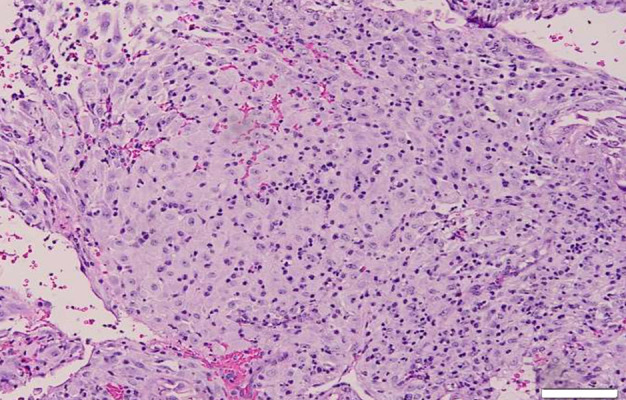
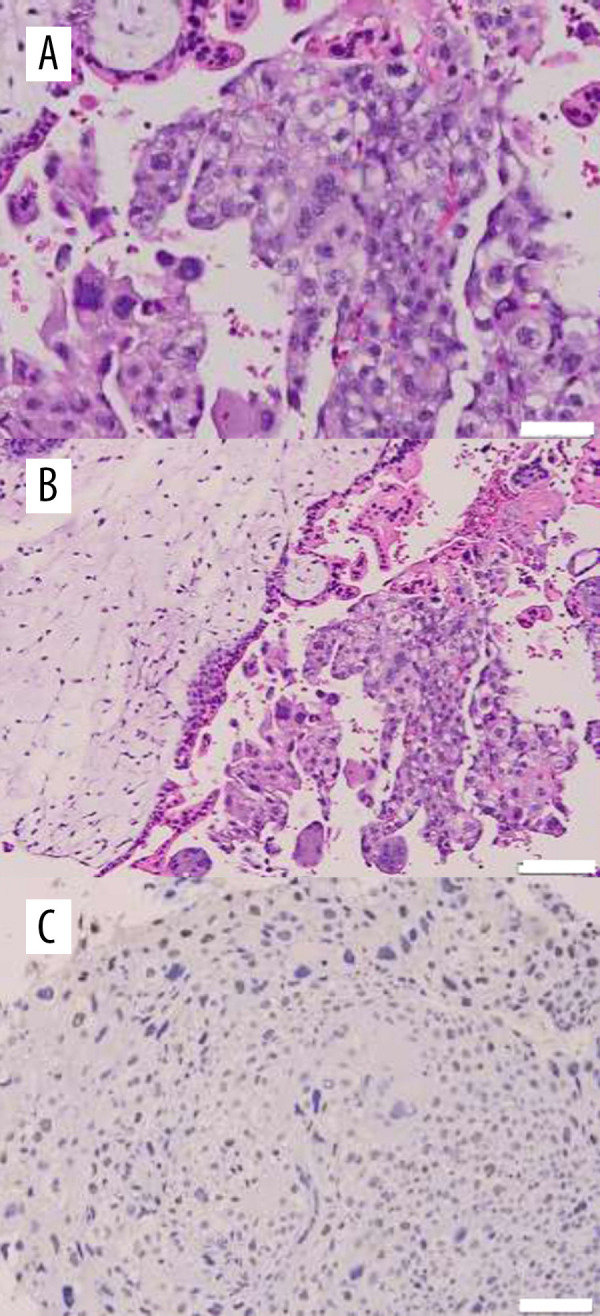
BACKGROUND Gestational trophoblastic disease (GTD) encompasses a group of disorders that arise from abnormal growth of trophoblastic tissue. The spectrum of GTD includes 2 major groups: benign and malignant. The benign form is a hydatidiform mole, either complete or partial; the malignant forms, referred to as gestational trophoblastic neoplasia (GTN), consist of invasive moles, choriocarcinomas, placental site trophoblastic tumors, and epithelioid trophoblastic tumors. Most patients who undergo evacuation of a hydatidiform mole by curettage have a disease-free period before a new tumor develops that can be considered malignant. In rare cases, metastasis occurs rapidly and manifests coincidentally before the hydatidiform mole can be evacuated. CASE REPORT A 19-year-old woman in Bandung City, West Java, Indonesia, was diagnosed with a molar pregnancy with early evidence of a mass in her vagina that was suspicious for stage II GTN. The early emergence of a vaginal mass was a rare case of early transformation of a molar pregnancy into GTN. CONCLUSIONS Careful evaluation is warranted of patients with characteristics typical of an intrauterine molar pregnancy who have an early presentation of a vaginal mass because of the possibility that the diagnosis could be GTN.
Conflict of interest statement
None.
Figures
Similar articles
-
A Case of Rapid Transformation from Hydatidiform Mole to Invasive Mole: The Importance of β-hCG (Human Chorionic Gonadotropin) Serum Levels in Follow-Up Evaluation.Am J Case Rep. 2021 Jun 15;22:e931156. doi: 10.12659/AJCR.931156. Am J Case Rep. 2021. PMID: 34127641 Free PMC article.
-
Surgery including fertility-sparing treatment of GTD.Best Pract Res Clin Obstet Gynaecol. 2021 Jul;74:97-108. doi: 10.1016/j.bpobgyn.2020.10.005. Epub 2020 Oct 10. Best Pract Res Clin Obstet Gynaecol. 2021. PMID: 33127305 Free PMC article. Review.
-
Gestational Trophoblastic Disease.2024 Feb 25. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2024 Feb 25. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 29261918 Free Books & Documents.
-
Advances in diagnostics and management of gestational trophoblastic disease.Radiol Oncol. 2022 Oct 27;56(4):430-439. doi: 10.2478/raon-2022-0038. eCollection 2022 Dec 1. Radiol Oncol. 2022. PMID: 36286620 Free PMC article. Review.
-
Pathology of Gestational Trophoblastic Disease (GTD).Hematol Oncol Clin North Am. 2024 Dec;38(6):1191-1217. doi: 10.1016/j.hoc.2024.08.017. Epub 2024 Sep 24. Hematol Oncol Clin North Am. 2024. PMID: 39322461 Review.
References
-
- Lurain JR. Gestational trophoblastic disease I: Epidemiology, pathology, clinical presentation and diagnosis of gestational trophoblastic disease, and management of hydatidiform mole. Am J Obstet Gynecol. 2010;203(6):531–39. - PubMed
-
- Tricia ME OQA. In: Gestational throphoblastic diseases. 9th ed. DeCherney AH NL, editor. Los Angeles: McGraw-Hill Companies; 2003.
-
- Bruce S, Sorosky J. StatPearls. Treasure Island (FL): StatPearls Publishing; 2021. Gestational trophoblastic disease. [Updated 2020 Aug 26] https://www.ncbi.nlm.nih.gov/books/NBK470267/ - PubMed
-
- Genest D, Berkowitz RS, Fisher RA, et al. Gestational trophoblastic disease. In: Tavassoli FA, Devilee P, editors. World Health Organization Classification of Tumours. Lyon: Tumors of the breast and female genital tract. IARC Press; 2003. pp. 250–54.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
