

Skull base repair following endonasal pituitary and skull base tumour resection: a systematic review
- PMID: 33973152
- PMCID: PMC8416859
- DOI: 10.1007/s11102-021-01145-4
Skull base repair following endonasal pituitary and skull base tumour resection: a systematic review
Abstract
Purpose: Postoperative cerebrospinal fluid rhinorrhoea (CSFR) remains a frequent complication of endonasal approaches to pituitary and skull base tumours. Watertight skull base reconstruction is important in preventing CSFR. We sought to systematically review the current literature of available skull base repair techniques.
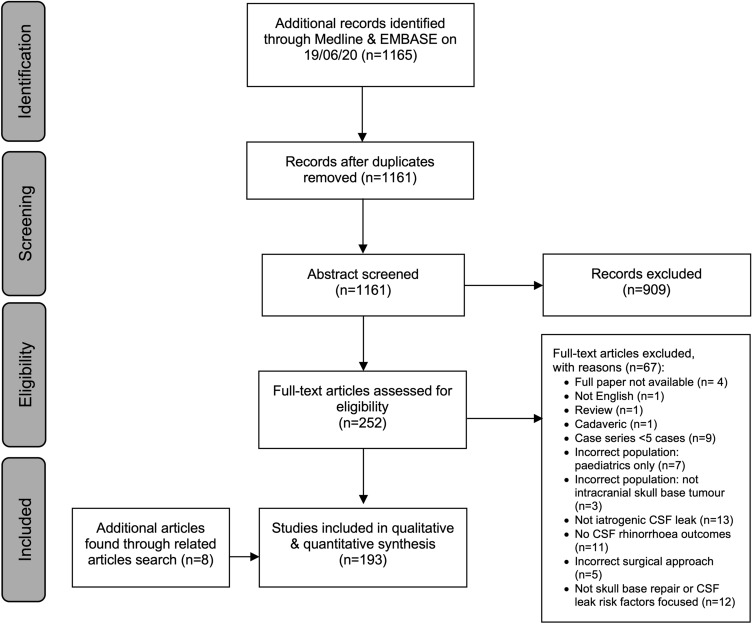
Methods: Pubmed and Embase databases were searched for studies (2000-2020) that (a) reported on the endonasal resection of pituitary and skull base tumours, (b) focussed on skull base repair techniques and/or postoperative CSFR risk factors, and (c) included CSFR data. Roles, advantages and disadvantages of each repair method were detailed. Random-effects meta-analyses were performed where possible.
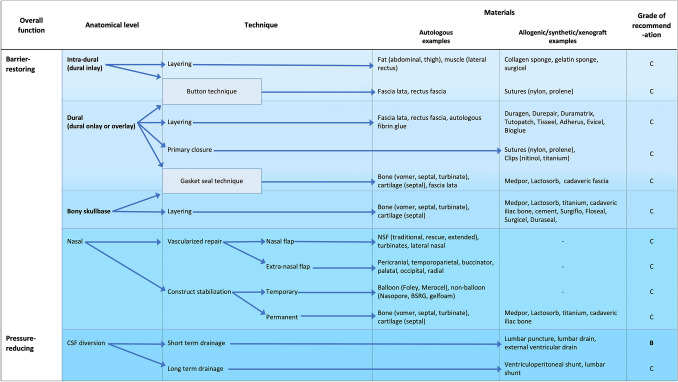
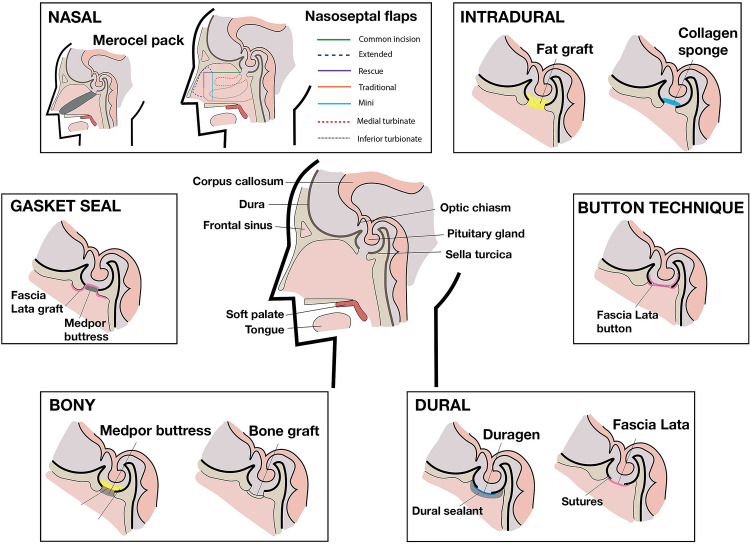
Results: 193 studies were included. Repair methods were categorised based on function and anatomical level. There was absolute heterogeneity in repair methods used, with no independent studies sharing the same repair protocol. Techniques most commonly used for low CSFR risk cases were fat grafts, fascia lata grafts and synthetic grafts. For cases with higher CSFR risk, multilayer regimes were utilized with vascularized flaps, gasket sealing and lumbar drains. Lumbar drain use for high CSFR risk cases was supported by a randomised study (Oxford CEBM: Grade B recommendation), but otherwise there was limited high-level evidence. Pooled CSFR incidence by approach was 3.7% (CI 3-4.5%) for transsphenoidal, 9% (CI 7.2-11.3%) for expanded endonasal, and 5.3% (CI 3.4-7%) for studies describing both. Further meaningful meta-analyses of repair methods were not performed due to significant repair protocol heterogeneity.
Conclusions: Modern reconstructive protocols are heterogeneous and there is limited evidence to suggest the optimal repair technique after pituitary and skull base tumour resection. Further studies are needed to guide practice.
Keywords: CSF; Cerebrospinal fluid; Cerebrospinal fluid leak; Cerebrospinal fluid rhinorrhoea; Endoscopic endonasal; Endoscopic transsphenoidal surgery; Skull base surgery.
© 2021. The Author(s).
Conflict of interest statement
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers' bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Figures
References
-
- Attia M, Kandasamy J, Jakimovski D, Bedrosian J, Alimi M, Lee DLY, et al. The importance and timing of optic canal exploration and decompression during endoscopic endonasal resection of tuberculum sella and planum sphenoidale meningiomas. Oper Neurosurg. 2012;71(suppl_1):ons58–ons67. doi: 10.1227/NEU.0b013e318258e23d. - DOI - PubMed
-
- Liu JK, Christiano LD, Patel SK, Tubbs RS, Eloy JA. Surgical nuances for removal of tuberculum sellae meningiomas with optic canal involvement using the endoscopic endonasal extended transsphenoidal transplanum transtuberculum approach. Neurosurg Focus. 2011;30(5):E2. doi: 10.3171/2011.3.FOCUS115. - DOI - PubMed
-
- Muskens IS, Briceno V, Ouwehand TL, Castlen JP, Gormley WB, Aglio LS, et al. The endoscopic endonasal approach is not superior to the microscopic transcranial approach for anterior skull base meningiomas: a meta-analysis. Acta Neurochir. 2018;160(1):59–75. doi: 10.1007/s00701-017-3390-y. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
