

Lorlatinib Exposure-Response Analyses for Safety and Efficacy in a Phase I/II Trial to Support Benefit-Risk Assessment in Non-Small Cell Lung Cancer
- PMID: 33973232
- PMCID: PMC9290079
- DOI: 10.1002/cpt.2228
Lorlatinib Exposure-Response Analyses for Safety and Efficacy in a Phase I/II Trial to Support Benefit-Risk Assessment in Non-Small Cell Lung Cancer
Abstract
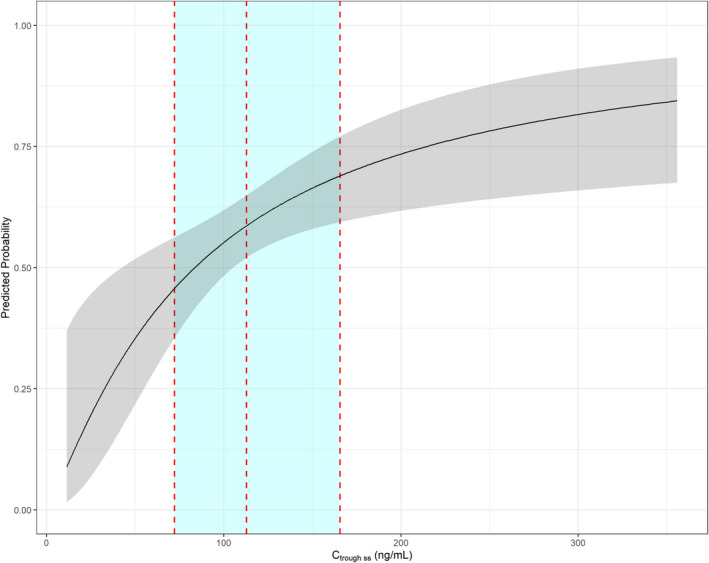
Lorlatinib is a small molecule inhibitor of anaplastic lymphoma kinase (ALK) and c-ROS oncogene 1 (ROS1) tyrosine kinases and is approved for the treatment of patients with ALK-positive advanced non-small cell lung cancer (NSCLC). In the phase I/II study (NCT01970865), potential exposure-response (E-R) relationships between lorlatinib and selected safety and efficacy end points were evaluated in patients with NSCLC. E-R relationships were assessed for safety end points with incidence > 10% in all treated patients (n = 328). In total, 4 safety end points were assessed: hypercholesterolemia grade ≥ 3, hypertriglyceridemia grade ≥ 3, weight gain grade ≥ 2, and treatment-emergent adverse events (TEAEs) grade ≥ 3. Using logistic regression, significant relationships were identified between lorlatinib plasma exposure and risk of hypercholesterolemia grade ≥ 3 (odds ratio (OR) 5.256) and risk of TEAE grade ≥ 3 (OR 3.214). The covariates baseline cholesterol and time on study prior to the event (TE) were associated with the probability of hypercholesterolemia grade ≥ 3. Baseline cholesterol and TE were found to have a statistically significant correlation with TEAE grade ≥ 3. Exposure-efficacy relationships were assessed for objective response rate (ORR; n = 197) and intracranial objective response rate (IC-ORR; n = 132). Lorlatinib plasma exposure was not identified as a statistically significant factor related to either efficacy end point. The only significant E-R relationships identified for efficacy were between baseline alkaline phosphatase and baseline amylase with IC-ORR (ORs 0.363 and 1.015, respectively). These findings support the lorlatinib indicated dose and dose modification guidelines regarding the management of lorlatinib-related AEs.
© 2021 Pfizer Inc. Clinical Pharmacology & Therapeutics published by Wiley Periodicals LLC on behalf of American Society for Clinical Pharmacology and Therapeutics.
Conflict of interest statement
J.C., A.R.‐G., L.P.J., G.P., H.T., J.C., and J.H. are current or former employees of Pfizer Inc.
Figures

Comment in
-
Response to "Lorlatinib Exposed: A Far from Optimal Dose".Clin Pharmacol Ther. 2022 Jun;111(6):1197-1198. doi: 10.1002/cpt.2580. Epub 2022 Mar 31. Clin Pharmacol Ther. 2022. PMID: 35358326 No abstract available.
-
Lorlatinib Exposed: A Far From Optimal Dose.Clin Pharmacol Ther. 2022 Jun;111(6):1195-1196. doi: 10.1002/cpt.2579. Epub 2022 Apr 8. Clin Pharmacol Ther. 2022. PMID: 35394660 No abstract available.
References
-
- Global Burden of Disease Cancer Collaboration . Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability‐adjusted life‐years for 29 cancer groups, 1990 to 2017: a systematic analysis for the global burden of disease study. JAMA Oncol. 5, 1749–1768 (2019). - PMC - PubMed
-
- Ferlay, J. et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 136, E359–E386 (2015). - PubMed
-
- American Cancer Society . Cancer facts & figures. The Society (2008).
-
- Rimkunas, V.M. et al. Analysis of receptor tyrosine kinase ROS1‐positive tumors in non‐small cell lung cancer: identification of a FIG‐ROS1 fusion. Clin. Cancer Res. 18, 4449–4457 (2012). - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
