

Deciphering the Efficacy and Mechanisms of Chinese Herbal Medicine for Diabetic Kidney Disease by Integrating Web-Based Biochemical Databases and Real-World Clinical Data: Retrospective Cohort Study
- PMID: 33973855
- PMCID: PMC8150407
- DOI: 10.2196/27614
Deciphering the Efficacy and Mechanisms of Chinese Herbal Medicine for Diabetic Kidney Disease by Integrating Web-Based Biochemical Databases and Real-World Clinical Data: Retrospective Cohort Study
Abstract
Background: Diabetic kidney disease (DKD) is one of the most crucial causes of chronic kidney disease (CKD). However, the efficacy and biomedical mechanisms of Chinese herbal medicine (CHM) for DKD in clinical settings remain unclear.
Objective: This study aimed to analyze the outcomes of DKD patients with CHM-only management and the possible molecular pathways of CHM by integrating web-based biomedical databases and real-world clinical data.
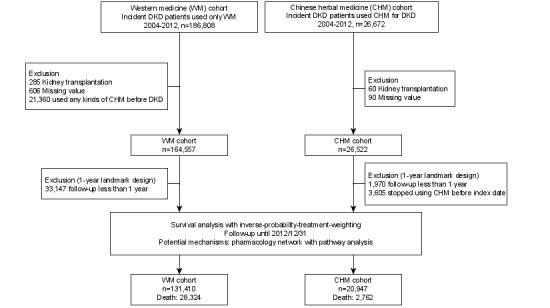
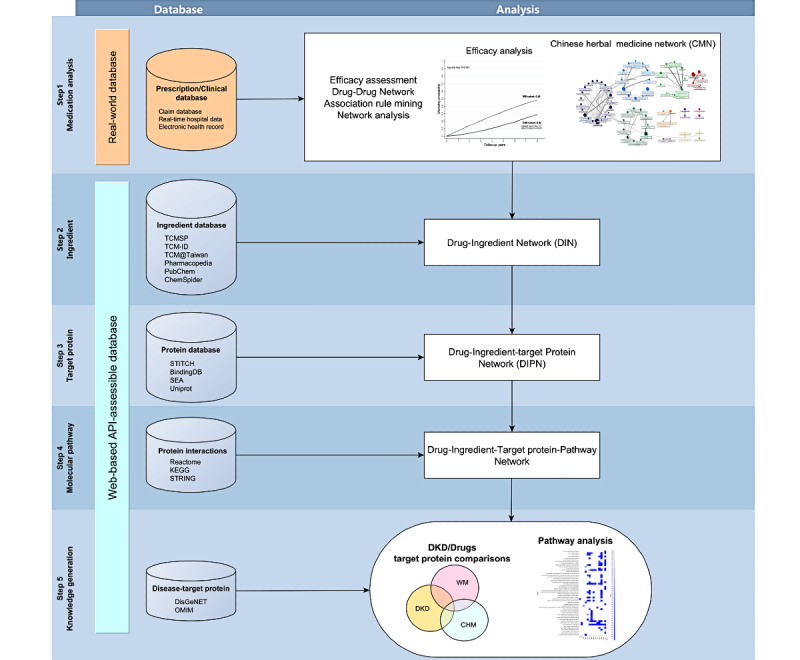
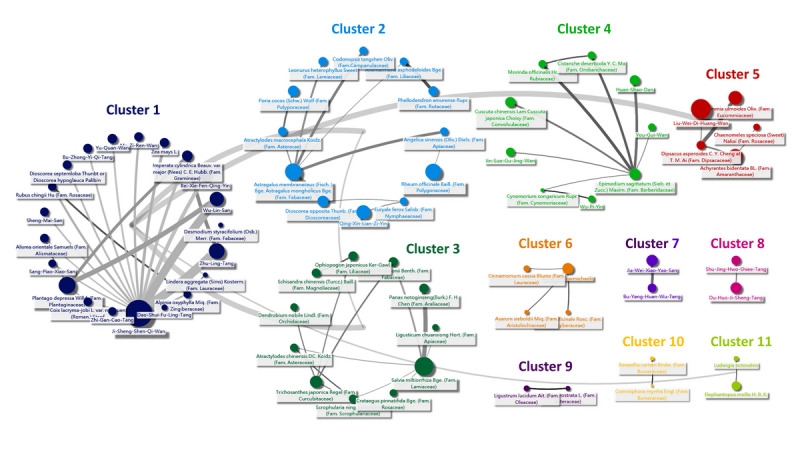
Methods: A total of 152,357 patients with incident DKD from 2004 to 2012 were identified from the National Health Insurance Research Database (NHIRD) in Taiwan. The risk of mortality was estimated with the Kaplan-Meier method and Cox regression considering demographic covariates. The inverse probability of treatment weighting was used for confounding bias between CHM users and nonusers. Furthermore, to decipher the CHM used for DKD, we analyzed all CHM prescriptions using the Chinese Herbal Medicine Network (CMN), which combined association rule mining and social network analysis for all CHM prescriptions. Further, web-based biomedical databases, including STITCH, STRING, BindingDB, TCMSP, TCM@Taiwan, and DisGeNET, were integrated with the CMN and commonly used Western medicine (WM) to explore the differences in possible target proteins and molecular pathways between CHM and WM. An application programming interface was used to assess these online databases to obtain the latest biomedical information.
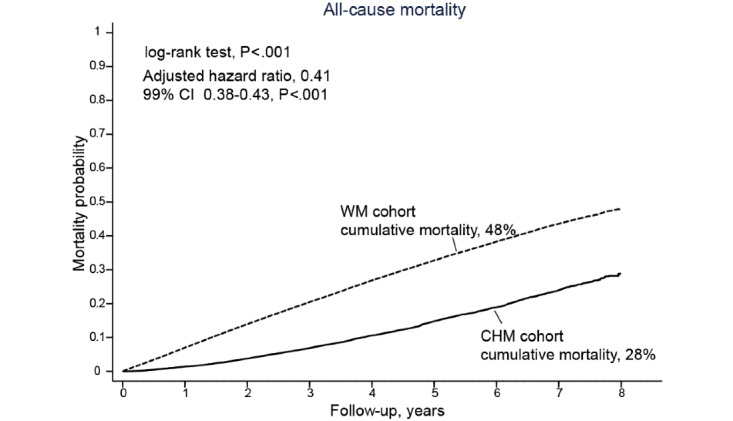
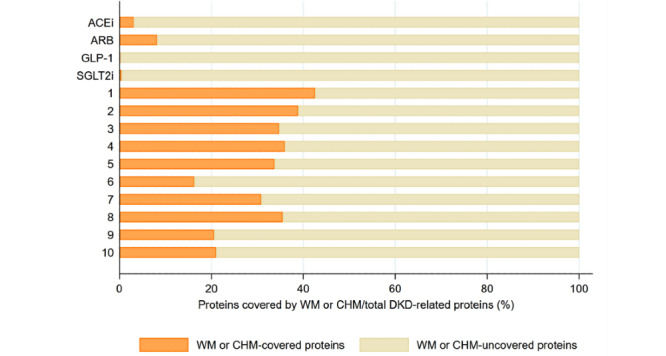
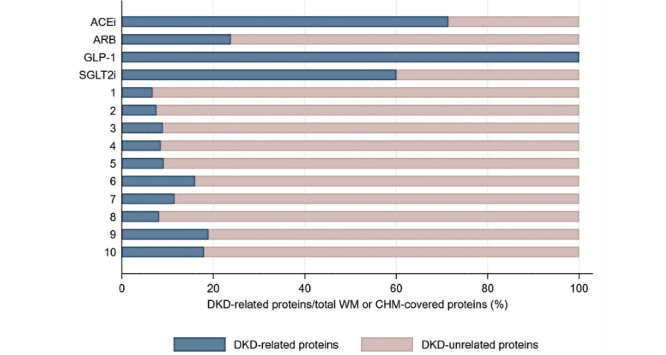
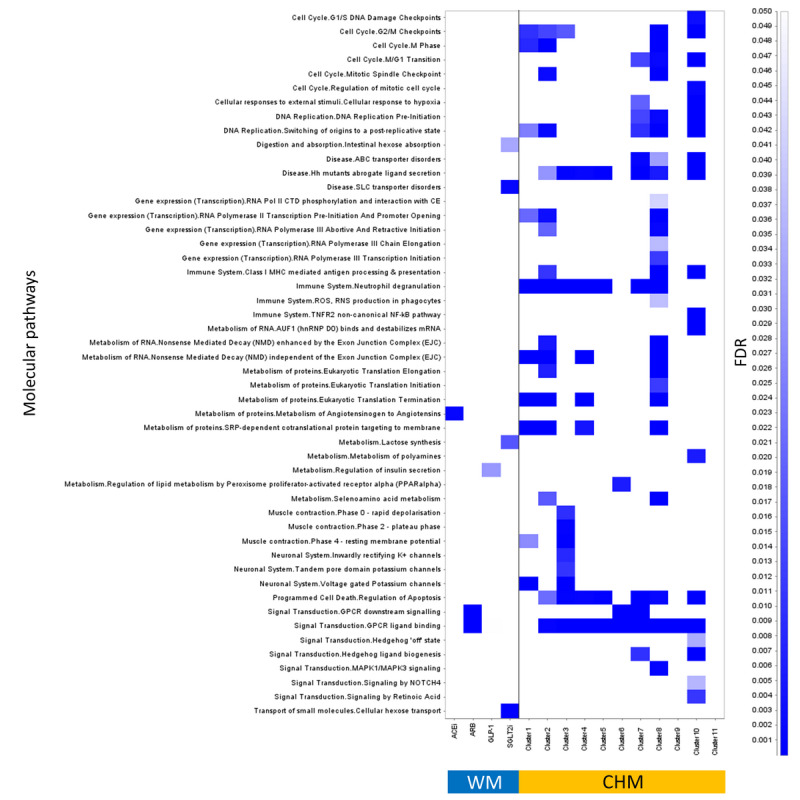
Results: About 13.7% (20,947/131,410) of patients were classified as CHM users among eligible DKD patients. The median follow-up duration of all patients was 2.49 years. The cumulative mortality rate in the CHM cohort was significantly lower than that in the WM cohort (28% vs 48%, P<.001). The risk of mortality was 0.41 in the CHM cohort with covariate adjustment (99% CI 0.38-0.43; P<.001). A total of 173,525 CHM prescriptions were used to construct the CMN with 11 CHM clusters. CHM covered more DKD-related proteins and pathways than WM; nevertheless, WM aimed at managing DKD more specifically. From the overrepresentation tests carried out by the online website Reactome, the molecular pathways covered by the CHM clusters in the CMN and WM seemed distinctive but complementary. Complementary effects were also found among DKD patients with concurrent WM and CHM use. The risk of mortality for CHM users under renin-angiotensin-aldosterone system (RAAS) inhibition therapy was lower than that for CHM nonusers among DKD patients with hypertension (adjusted hazard ratio [aHR] 0.47, 99% CI 0.45-0.51; P<.001), chronic heart failure (aHR 0.43, 99% CI 0.37-0.51; P<.001), and ischemic heart disease (aHR 0.46, 99% CI 0.41-0.51; P<.001).
Conclusions: CHM users among DKD patients seemed to have a lower risk of mortality, which may benefit from potentially synergistic renoprotection effects. The framework of integrating real-world clinical databases and web-based biomedical databases could help in exploring the roles of treatments for diseases.
Keywords: Chinese medicine network; association rule mining; social network analysis; survival.
©Chien-Wei Wu, Hsing-Yu Chen, Ching-Wei Yang, Yu-Chun Chen. Originally published in JMIR Medical Informatics (https://medinform.jmir.org), 11.05.2021.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Tsai S, Tseng H, Tan H, Chien Y, Chang C. End-stage renal disease in Taiwan: a case-control study. J Epidemiol. 2009;19(4):169–76. doi: 10.2188/jea.je20080099. http://joi.jlc.jst.go.jp/JST.JSTAGE/jea/JE20080099?from=PubMed - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
