

Transforming a Patient Registry Into a Customized Data Set for the Advanced Statistical Analysis of Health Risk Factors and for Medication-Related Hospitalization Research: Retrospective Hospital Patient Registry Study
- PMID: 33973865
- PMCID: PMC8150425
- DOI: 10.2196/24205
Transforming a Patient Registry Into a Customized Data Set for the Advanced Statistical Analysis of Health Risk Factors and for Medication-Related Hospitalization Research: Retrospective Hospital Patient Registry Study
Abstract
Background: Hospital patient registries provide substantial longitudinal data sets describing the clinical and medical health statuses of inpatients and their pharmacological prescriptions. Despite the multiple advantages of routinely collecting multidimensional longitudinal data, those data sets are rarely suitable for advanced statistical analysis and they require customization and synthesis.
Objective: The aim of this study was to describe the methods used to transform and synthesize a raw, multidimensional, hospital patient registry data set into an exploitable database for the further investigation of risk profiles and predictive and survival health outcomes among polymorbid, polymedicated, older inpatients in relation to their medicine prescriptions at hospital discharge.
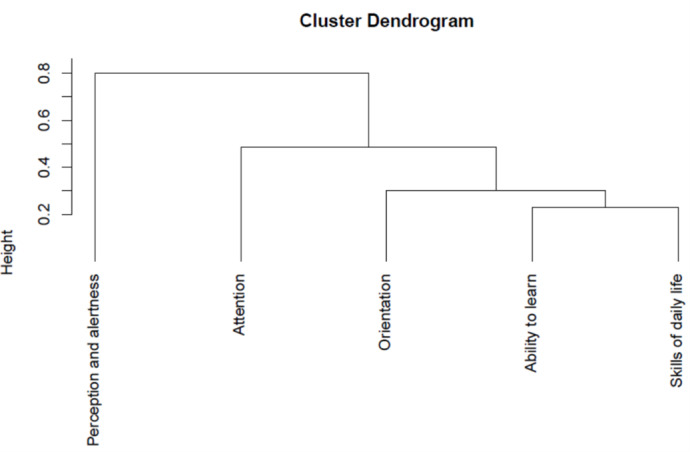
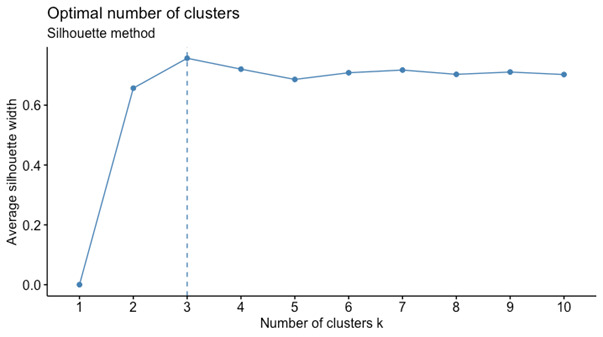
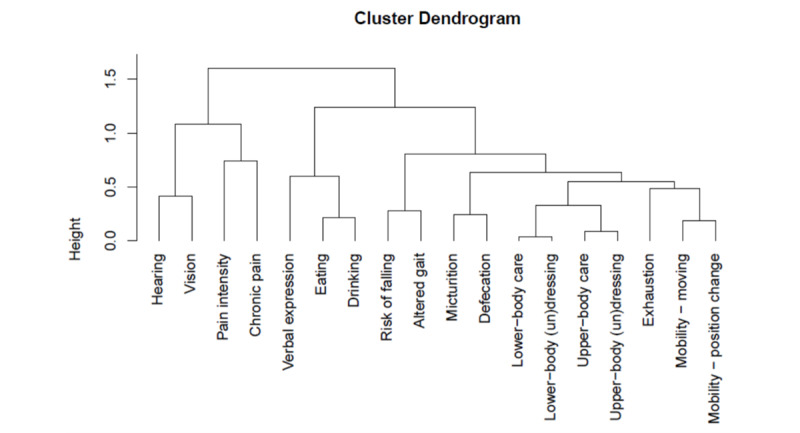
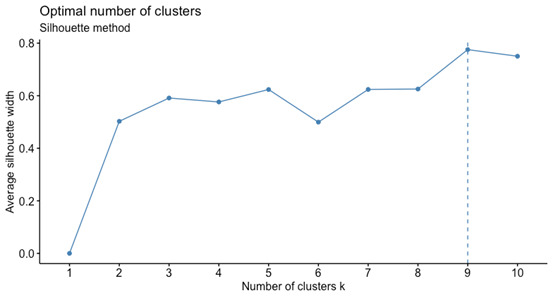
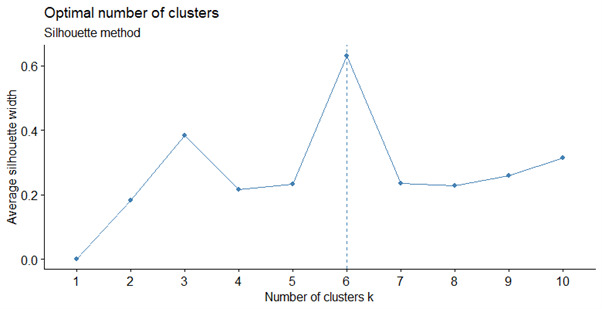
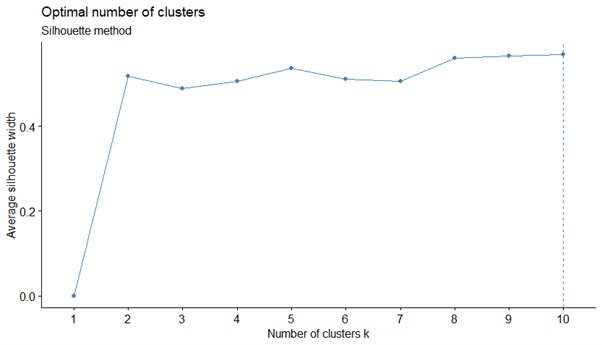
Methods: A raw, multidimensional data set from a public hospital was extracted from the hospital registry in a CSV (.csv) file and imported into the R statistical package for cleaning, customization, and synthesis. Patients fulfilling the criteria for inclusion were home-dwelling, polymedicated, older adults with multiple chronic conditions aged ≥65 who became hospitalized. The patient data set covered 140 variables from 20,422 hospitalizations of polymedicated, home-dwelling older adults from 2015 to 2018. Each variable, according to type, was explored and computed to describe distributions, missing values, and associations. Different clustering methods, expert opinion, recoding, and missing-value techniques were used to customize and synthesize these multidimensional data sets.
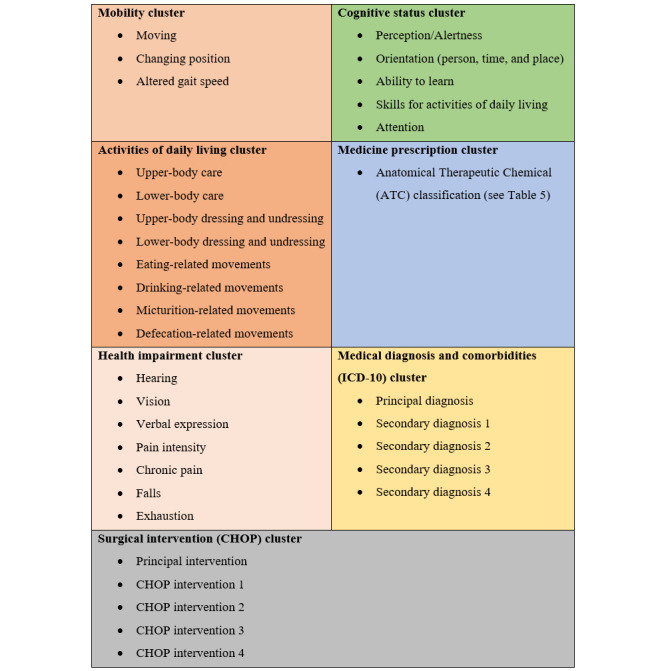
Results: Sociodemographic data showed no missing values. Average age, hospital length of stay, and frequency of hospitalization were computed. Discharge details were recoded and summarized. Clinical data were cleaned up and best practices for managing missing values were applied. Seven clusters of medical diagnoses, surgical interventions, somatic, cognitive, and medicines data were extracted using empirical and statistical best practices, with each presenting the health status of the patients included in it as accurately as possible. Medical, comorbidity, and drug data were recoded and summarized.
Conclusions: A cleaner, better-structured data set was obtained, combining empirical and best-practice statistical approaches. The overall strategy delivered an exploitable, population-based database suitable for an advanced analysis of the descriptive, predictive, and survival statistics relating to polymedicated, home-dwelling older adults admitted as inpatients. More research is needed to develop best practices for customizing and synthesizing large, multidimensional, population-based registries.
International registered report identifier (irrid): RR2-10.1136/bmjopen-2019-030030.
Keywords: cluster analysis; hierarchical 2-step clustering; hospital; multidimensional; population based; raw data; registry; retrospective.
©Zhivko Taushanov, Henk Verloo, Boris Wernli, Saviana Di Giovanni, Armin von Gunten, Filipa Pereira. Originally published in JMIR Medical Informatics (https://medinform.jmir.org), 11.05.2021.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
Similar articles
-
Development of a patient-centred medication management model for polymedicated home-dwelling older adults after hospital discharge: results of a mixed methods study.BMJ Open. 2023 Sep 20;13(9):e072738. doi: 10.1136/bmjopen-2023-072738. BMJ Open. 2023. PMID: 37730411 Free PMC article.
-
Optimising medication management for polymedicated home-dwelling older adults with multiple chronic conditions: a mixed-methods study protocol.BMJ Open. 2019 Oct 28;9(10):e030030. doi: 10.1136/bmjopen-2019-030030. BMJ Open. 2019. PMID: 31662367 Free PMC article.
-
Functional Status among Polymedicated Geriatric Inpatients at Discharge: A Population-Based Hospital Register Analysis.Geriatrics (Basel). 2021 Sep 3;6(3):86. doi: 10.3390/geriatrics6030086. Geriatrics (Basel). 2021. PMID: 34562987 Free PMC article.
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) acute day hospital versus admission; (2) vocational rehabilitation; (3) day hospital versus outpatient care.Health Technol Assess. 2001;5(21):1-75. doi: 10.3310/hta5210. Health Technol Assess. 2001. PMID: 11532238 Review.
-
The impact of transitional care programs on health services utilization in community-dwelling older adults: a systematic review.JBI Database System Rev Implement Rep. 2018 Feb;16(2):345-384. doi: 10.11124/JBISRIR-2017-003486. JBI Database System Rev Implement Rep. 2018. PMID: 29419621
Cited by
-
Using Existing Clinical Data to Measure Older Adult Inpatients' Frailty at Admission and Discharge: Hospital Patient Register Study.JMIR Aging. 2024 Oct 28;7:e54839. doi: 10.2196/54839. JMIR Aging. 2024. PMID: 39467281 Free PMC article.
-
Development of a patient-centred medication management model for polymedicated home-dwelling older adults after hospital discharge: results of a mixed methods study.BMJ Open. 2023 Sep 20;13(9):e072738. doi: 10.1136/bmjopen-2023-072738. BMJ Open. 2023. PMID: 37730411 Free PMC article.
-
Risk of 30-day hospital readmission associated with medical conditions and drug regimens of polymedicated, older inpatients discharged home: a registry-based cohort study.BMJ Open. 2021 Jul 14;11(7):e052755. doi: 10.1136/bmjopen-2021-052755. BMJ Open. 2021. PMID: 34261693 Free PMC article.
-
Prevalence and Early Prediction of Diabetes Using Machine Learning in North Kashmir: A Case Study of District Bandipora.Comput Intell Neurosci. 2022 Oct 4;2022:2789760. doi: 10.1155/2022/2789760. eCollection 2022. Comput Intell Neurosci. 2022. PMID: 36238678 Free PMC article.
-
Unplanned nursing home admission among discharged polymedicated older inpatients: a single-centre, registry-based study in Switzerland.BMJ Open. 2022 Mar 4;12(3):e057444. doi: 10.1136/bmjopen-2021-057444. BMJ Open. 2022. PMID: 35246423 Free PMC article.
References
-
- Gliklich R, Dreyer N, Leavy M. Registries for Evaluating Patient Outcomes: Patient Registries (3rd ed) Rockville, MD: Agency for Healthcare Research and Quality; 2014. - PubMed
-
- Brooke E. The current and future use of registers in health information systems. World Health Organization: Geneva. 1974:43. https://apps.who.int/iris/handle/10665/36936
-
- Walsh K, Marsolo Keith A, Davis Cori, Todd Theresa, Martineau Bernadette, Arbaugh Carlie, Verly Frederique, Samson Charles, Margolis Peter. Accuracy of the medication list in the electronic health record-implications for care, research, and improvement. J Am Med Inform Assoc. 2018 Jul 01;25(7):909–912. doi: 10.1093/jamia/ocy027. http://europepmc.org/abstract/MED/29771350 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
