

The Role of Primary Care in the Initiation of Opioid Use Disorder Treatment in Statewide Public and Private Insurance
- PMID: 33973922
- PMCID: PMC8578588
- DOI: 10.1097/ADM.0000000000000860
The Role of Primary Care in the Initiation of Opioid Use Disorder Treatment in Statewide Public and Private Insurance
Abstract
Objective: To determine if individuals newly diagnosed with opioid use disorder (OUD) who saw a primary care provider (PCP) before or on the date of diagnosis had higher rates of medication treatment for OUD (MOUD).
Methods: Observational study using logistic regression with claims data from Medicaid and a large private insurer in North Carolina from January 2014 to July 2017.
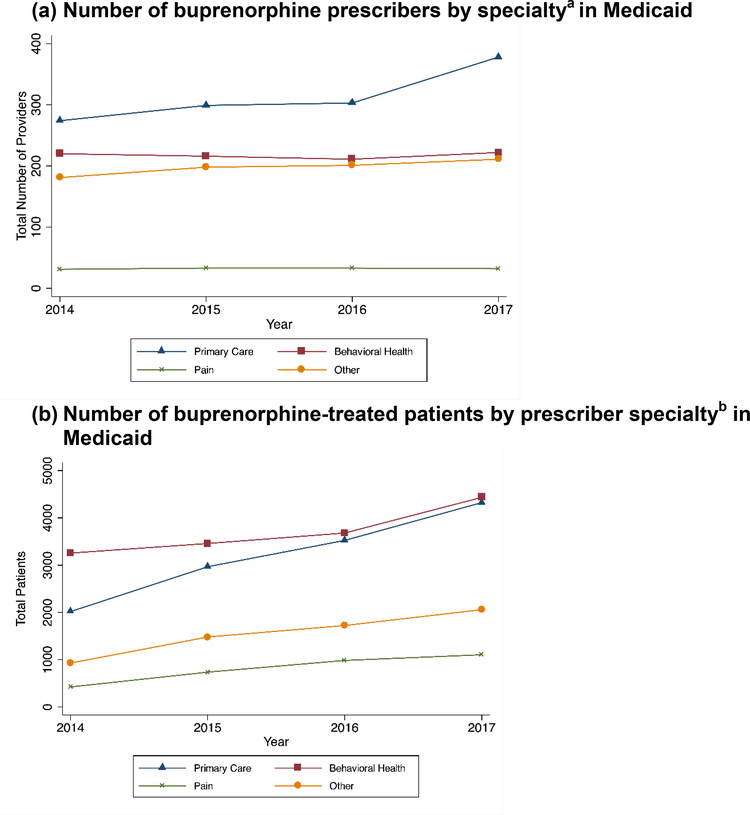
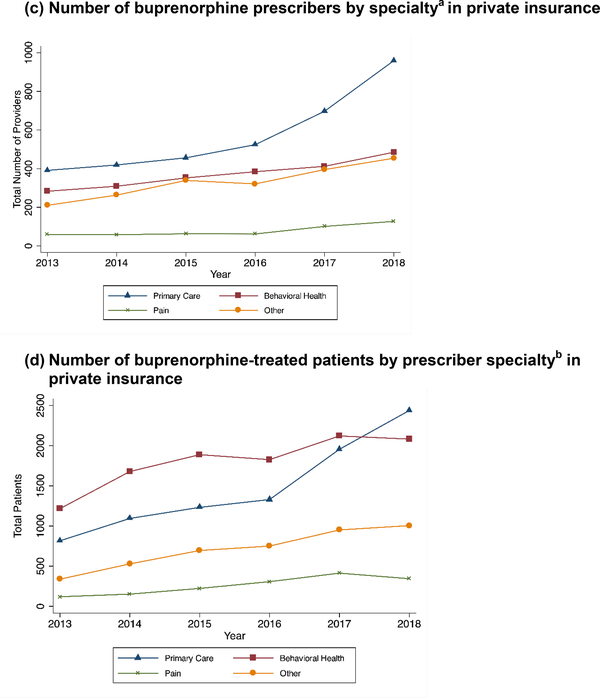
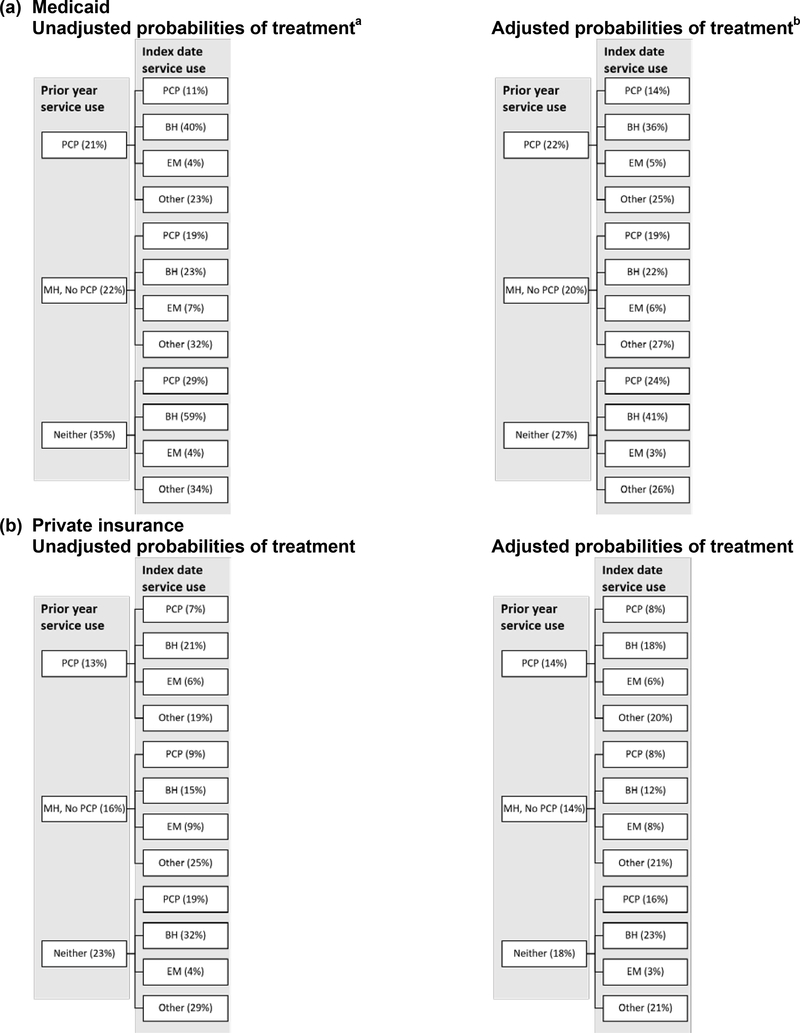
Key results: Between 2014 and 2017, the prevalence of diagnosed OUD increased by 47% among Medicaid enrollees and by 76% among the privately insured. Over the same time period, the percent of people with an OUD who received MOUD fell among both groups, while PCP involvement in treatment increased. Of Medicaid enrollees receiving buprenorphine, the percent receiving buprenorphine from a PCP increased from 32% in 2014 to 39% in 2017. Approximately 82% of people newly diagnosed with OUD had a PCP visit in the 12 months before diagnosis in Medicaid and private insurance. Those with a prior PCP visit were not more likely to receive MOUD. Seeing a PCP at diagnosis was associated with a higher probability of receiving MOUD than seeing an emergency provider but a lower probability than seeing a behavioral health specialist or other provider type.
Conclusions: People newly diagnosed with OUD had high rates of contact with PCPs before diagnosis, supporting the importance of PCPs in diagnosing OUD and connecting people to MOUD. Policies and programs to increase access to MOUD and improve PCPs' ability to connect people to evidence-based treatment are needed.
Copyright © 2021 American Society of Addiction Medicine.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
Similar articles
-
The Role of Primary Care in Improving Access to Medication-Assisted Treatment for Rural Medicaid Enrollees with Opioid Use Disorder.J Gen Intern Med. 2019 Jun;34(6):936-943. doi: 10.1007/s11606-019-04943-6. Epub 2019 Mar 18. J Gen Intern Med. 2019. PMID: 30887440 Free PMC article.
-
Are North Carolina clinicians delivering opioid use disorder treatment to Medicaid beneficiaries?Addiction. 2022 Nov;117(11):2855-2863. doi: 10.1111/add.15854. Epub 2022 Mar 7. Addiction. 2022. PMID: 35194878 Free PMC article.
-
Association of polysubstance use disorder with treatment quality among Medicaid beneficiaries with opioid use disorder.J Subst Abuse Treat. 2023 Jan;144:108921. doi: 10.1016/j.jsat.2022.108921. Epub 2022 Oct 27. J Subst Abuse Treat. 2023. PMID: 36327615 Free PMC article.
-
The cascade of care for opioid use disorder among youth in British Columbia, 2018.J Subst Abuse Treat. 2021 Nov;130:108404. doi: 10.1016/j.jsat.2021.108404. Epub 2021 Apr 18. J Subst Abuse Treat. 2021. PMID: 34118696 Review.
-
Management of opioid withdrawal and initiation of medications for opioid use disorder in the hospital setting.Hosp Pract (1995). 2022 Oct;50(4):251-258. doi: 10.1080/21548331.2022.2102776. Epub 2022 Jul 22. Hosp Pract (1995). 2022. PMID: 35837678 Review.
Cited by
-
Expanding access to medication treatment for opioid use disorders: Findings from the Washington State hub and spoke effort.Drug Alcohol Depend. 2024 Mar 1;256:111125. doi: 10.1016/j.drugalcdep.2024.111125. Epub 2024 Feb 14. Drug Alcohol Depend. 2024. PMID: 38368666 Free PMC article.
-
A study protocol for Project I-Test: a cluster randomized controlled trial of a practice coaching intervention to increase HIV testing in substance use treatment programs.Res Sq [Preprint]. 2023 Jun 28:rs.3.rs-3059783. doi: 10.21203/rs.3.rs-3059783/v1. Res Sq. 2023. Update in: Trials. 2023 Sep 26;24(1):609. doi: 10.1186/s13063-023-07602-8. PMID: 37461594 Free PMC article. Updated. Preprint.
-
Trauma Exposure Across the Lifespan among Individuals Engaged in Treatment with Medication for Opioid Use Disorder: Differences by Gender, PTSD Status, and Chronic Pain.Res Sq [Preprint]. 2023 Dec 19:rs.3.rs-3750143. doi: 10.21203/rs.3.rs-3750143/v1. Res Sq. 2023. Update in: Subst Abuse Treat Prev Policy. 2024 May 3;19(1):25. doi: 10.1186/s13011-024-00608-8. PMID: 38196650 Free PMC article. Updated. Preprint.
-
Trauma exposure across the lifespan among individuals engaged in treatment with medication for opioid use disorder: differences by gender, PTSD status, and chronic pain.Subst Abuse Treat Prev Policy. 2024 May 3;19(1):25. doi: 10.1186/s13011-024-00608-8. Subst Abuse Treat Prev Policy. 2024. PMID: 38702783 Free PMC article. Clinical Trial.
-
A study protocol for Project I-Test: a cluster randomized controlled trial of a practice coaching intervention to increase HIV testing in substance use treatment programs.Trials. 2023 Sep 26;24(1):609. doi: 10.1186/s13063-023-07602-8. Trials. 2023. PMID: 37749635 Free PMC article.
References
-
- Morgan JR, Schackman BR, Leff JA, Linas BP, Walley AY. Injectable naltrexone, oral naltrexone, and buprenorphine utilization and discontinuation among individuals treated for opioid use disorder in a United States commercially insured population HHS Public Access. J Subst Abus Treat. 2018;85:90–96. doi:10.1016/j.jsat.2017.07.001 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
