

Payment Discrepancies and Access to Primary Care Physicians for Dual-eligible Medicare-Medicaid Beneficiaries
- PMID: 33973937
- PMCID: PMC8486346
- DOI: 10.1097/MLR.0000000000001525
Payment Discrepancies and Access to Primary Care Physicians for Dual-eligible Medicare-Medicaid Beneficiaries
Abstract
Background: Physicians often receive lower payments for dual-eligible Medicare-Medicaid beneficiaries versus nondual Medicare beneficiaries because of state reimbursement caps. The Affordable Care Act (ACA) primary care fee bump temporarily eliminated this differential in 2013-2014.
Objective: To examine how dual payment policy impacts primary care physicians' (PCP) acceptance of duals.
Research design: We assessed differences in the likelihood that PCPs had dual caseloads of ≥10% or 20% in states with lower versus full dual reimbursement using linear probability models adjusted for physician and area-level traits. Using a triple-difference approach, we examined changes in dual caseloads for PCPs versus a control group of specialists in states with fee bumps versus no change during years postbump versus prebump.
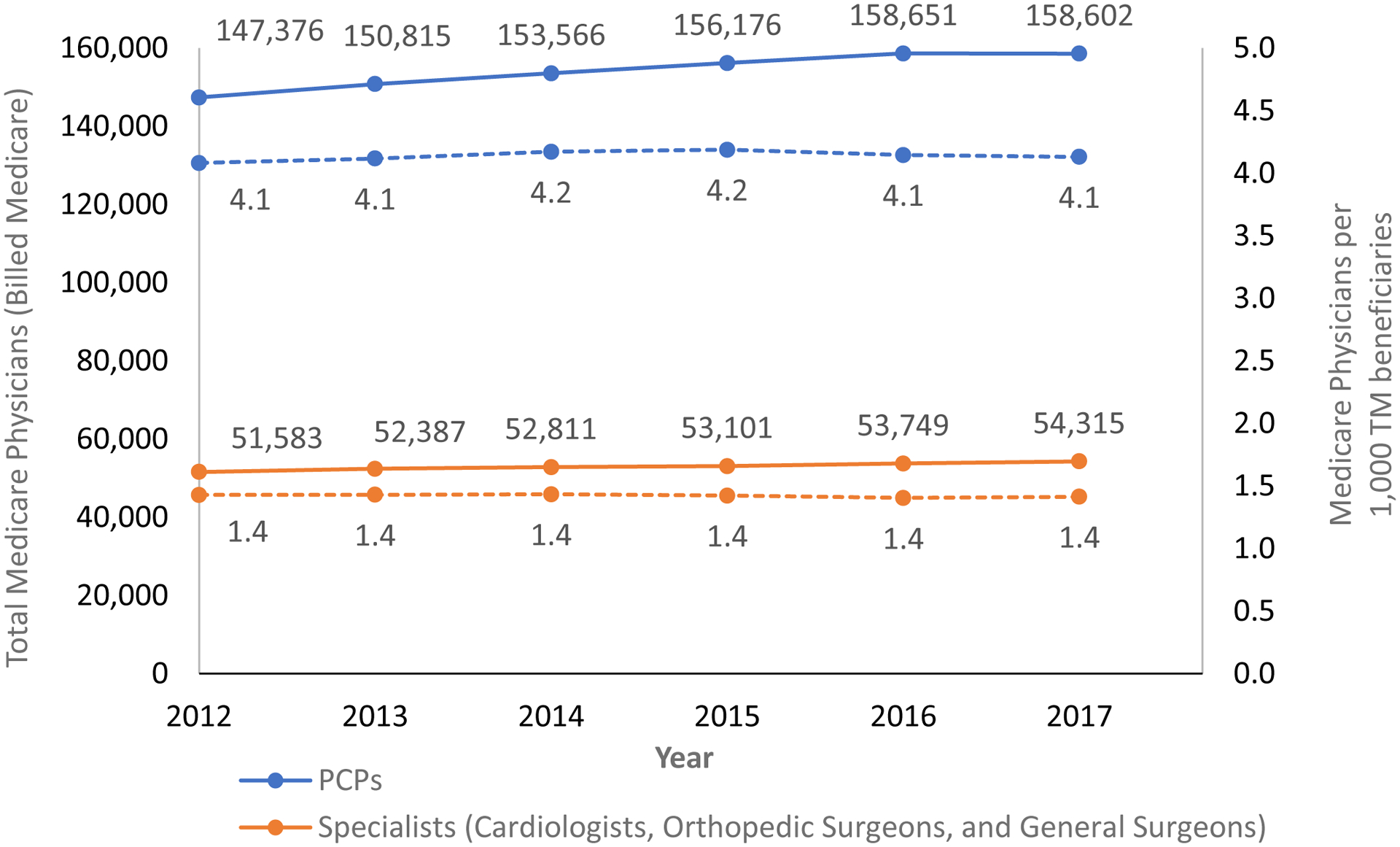
Subjects: PCPs and specialists (cardiologists, orthopedic surgeons, general surgeons) that billed fee-for-service Medicare.
Measures: State dual payment policies and physicians' dual caseloads as a percentage of their Medicare patients.
Results: In 2012, 81% of PCPs had dual caseloads of ≥10% and this was less likely among PCPs in states with lower versus full dual reimbursement (eg, difference=-4.52 percentage points; 95% confidence interval, -6.80 to -2.25). The proportion of PCPs with dual caseloads of ≥10% or 20% decreased significantly between 2012 and 2017 and the fee bump was not consistently associated with increases in dual caseloads.
Conclusions: Pre-ACA, PCPs' participation in the dual program appeared to be lower in states with lower reimbursement for duals. Despite the ACA fee bump, dual caseloads declined over time, raising concerns of worsening access to care.
Copyright © 2021 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
J.P.N. discloses that he was a director of Aetna until May 2018, held Aetna stock until November 2018, and currently owns stock in Novartis and Medtronic. There are no other relevant disclosures. The remaining authors declare no conflict of interest.
Figures

References
-
- Congressional Budget Office. Dual-Eligible Beneficiaries of Medicare and Medicaid: Characteristics, Health Care Spending, and Evolving Policies. June2013. Available at: https://www.cbo.gov/sites/default/files/113th-congress-2013-2014/reports....AccessedJuly 19, 2020.
-
- Medicaid and CHIP Payment and Access Commission. Effects of Medicaid Coverage of Medicare Cost Sharing on Access to Care. March2015. Available at: https://www.macpac.gov/wp-content/uploads/2015/03/Effects-of-Medicaid-Co....AccessedJuly 19, 2020.
-
- Kaiser Familty Foundation. Medicaid-to-Medicare Fee Index. 2016. Available at: https://www.kff.org/medicaid/state-indicator/medicaid-to-medicare-fee-in....AccessedJuly 19, 2020.
-
- Berman S, Dolins J, Tang S-f, Yudkowsky B. Factors that influence the willingness of private primary care pediatricians to accept more Medicaid patients. Pediatrics 2002;110(2):239–248. - PubMed
-
- Zuckerman S, McFeeters J, Cunningham P, Nichols L. Changes in medicaid physician fees, 1998–2003: implications for physician participation. Health Aff (Millwood) 2004;23:W4–374 – W4–384. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
