

Effect of Antimicrobial Therapy on Respiratory Hospitalization or Death in Adults With Idiopathic Pulmonary Fibrosis: The CleanUP-IPF Randomized Clinical Trial
- PMID: 33974018
- PMCID: PMC8114133
- DOI: 10.1001/jama.2021.4956
Effect of Antimicrobial Therapy on Respiratory Hospitalization or Death in Adults With Idiopathic Pulmonary Fibrosis: The CleanUP-IPF Randomized Clinical Trial
Abstract
Importance: Alteration in lung microbes is associated with disease progression in idiopathic pulmonary fibrosis.
Objective: To assess the effect of antimicrobial therapy on clinical outcomes.
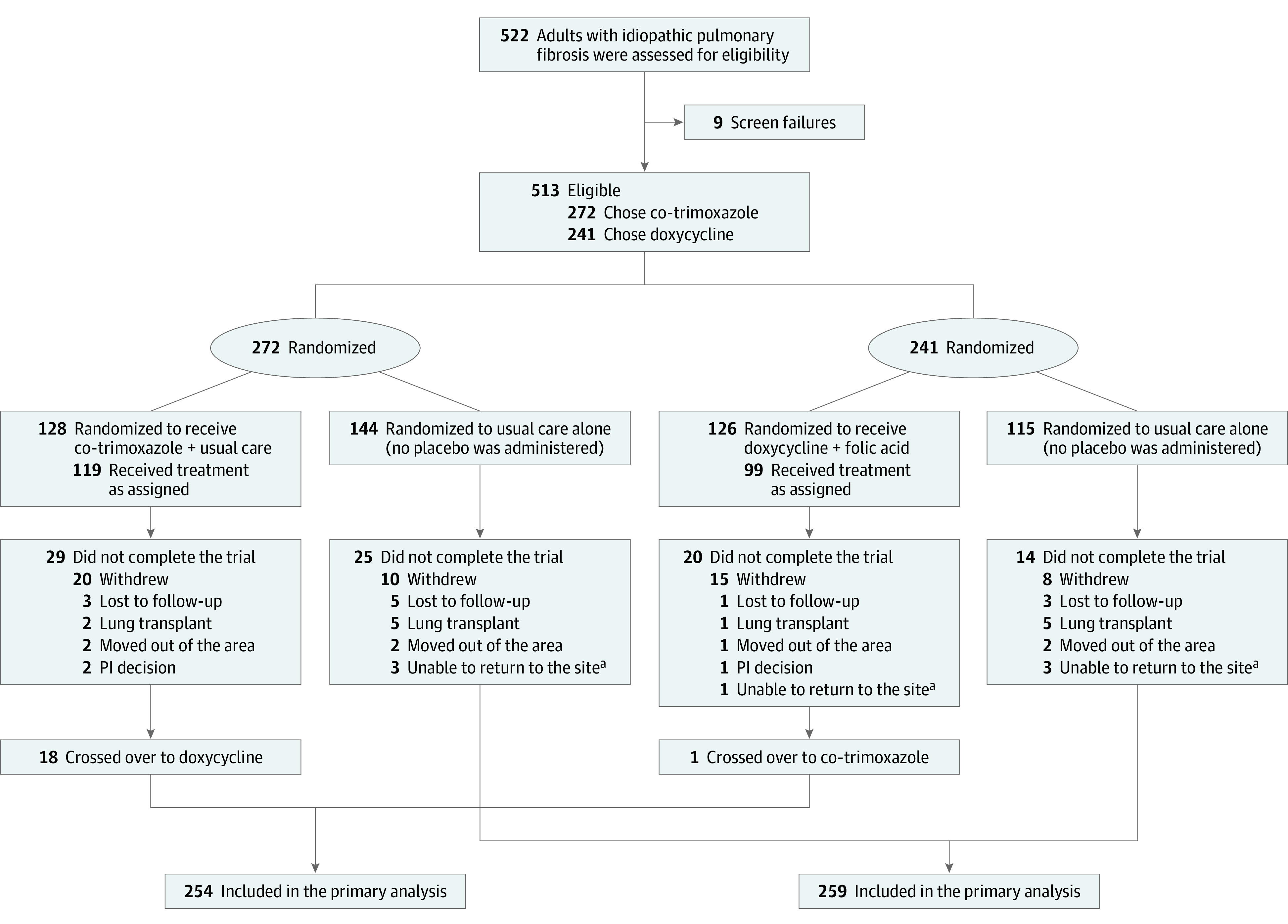
Design, setting, and participants: Pragmatic, randomized, unblinded clinical trial conducted across 35 US sites. A total of 513 patients older than 40 years were randomized from August 2017 to June 2019 (final follow-up was January 2020).
Interventions: Patients were randomized in a 1:1 allocation ratio to receive antimicrobials (n = 254) or usual care alone (n = 259). Antimicrobials included co-trimoxazole (trimethoprim 160 mg/sulfamethoxazole 800 mg twice daily plus folic acid 5 mg daily, n = 128) or doxycycline (100 mg once daily if body weight <50 kg or 100 mg twice daily if ≥50 kg, n = 126). No placebo was administered in the usual care alone group.
Main outcomes and measures: The primary end point was time to first nonelective respiratory hospitalization or all-cause mortality.
Results: Among the 513 patients who were randomized (mean age, 71 years; 23.6% women), all (100%) were included in the analysis. The study was terminated for futility on December 18, 2019. After a mean follow-up time of 13.1 months (median, 12.7 months), a total of 108 primary end point events occurred: 52 events (20.4 events per 100 patient-years [95% CI, 14.8-25.9]) in the usual care plus antimicrobial therapy group and 56 events (18.4 events per 100 patient-years [95% CI, 13.2-23.6]) in the usual care group, with no significant difference between groups (adjusted HR, 1.04 [95% CI, 0.71-1.53; P = .83]. There was no statistically significant interaction between the effect of the prespecified antimicrobial agent (co-trimoxazole vs doxycycline) on the primary end point (adjusted HR, 1.15 [95% CI 0.68-1.95] in the co-trimoxazole group vs 0.82 [95% CI, 0.46-1.47] in the doxycycline group; P = .66). Serious adverse events occurring at 5% or greater among those treated with usual care plus antimicrobials vs usual care alone included respiratory events (16.5% vs 10.0%) and infections (2.8% vs 6.6%); adverse events of special interest included diarrhea (10.2% vs 3.1%) and rash (6.7% vs 0%).
Conclusions and relevance: Among adults with idiopathic pulmonary fibrosis, the addition of co-trimoxazole or doxycycline to usual care, compared with usual care alone, did not significantly improve time to nonelective respiratory hospitalization or death. These findings do not support treatment with these antibiotics for the underlying disease.
Trial registration: ClinicalTrials.gov Identifier: NCT02759120.
Conflict of interest statement
Figures

Comment in
-
Antimicrobial Therapy and Respiratory Hospitalization or Death in Adults With Idiopathic Pulmonary Fibrosis.JAMA. 2021 Sep 21;326(11):1070-1071. doi: 10.1001/jama.2021.11810. JAMA. 2021. PMID: 34546305 No abstract available.
-
New Frontiers in Therapeutics for Interstitial Lung Diseases.Am J Respir Crit Care Med. 2023 Apr 15;207(8):1089-1091. doi: 10.1164/rccm.202206-1035RR. Am J Respir Crit Care Med. 2023. PMID: 36735934 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
