

Effect of an Internet-Delivered Stepped-Care Program vs In-Person Cognitive Behavioral Therapy on Obsessive-Compulsive Disorder Symptoms in Children and Adolescents: A Randomized Clinical Trial
- PMID: 33974020
- PMCID: PMC8114140
- DOI: 10.1001/jama.2021.3839
Effect of an Internet-Delivered Stepped-Care Program vs In-Person Cognitive Behavioral Therapy on Obsessive-Compulsive Disorder Symptoms in Children and Adolescents: A Randomized Clinical Trial
Abstract
Importance: In most countries, young people with obsessive-compulsive disorder have limited access to specialist cognitive behavioral therapy (CBT), a first-line treatment.
Objective: To investigate whether internet-delivered CBT implemented in a stepped-care model is noninferior to in-person CBT for pediatric obsessive-compulsive disorder.
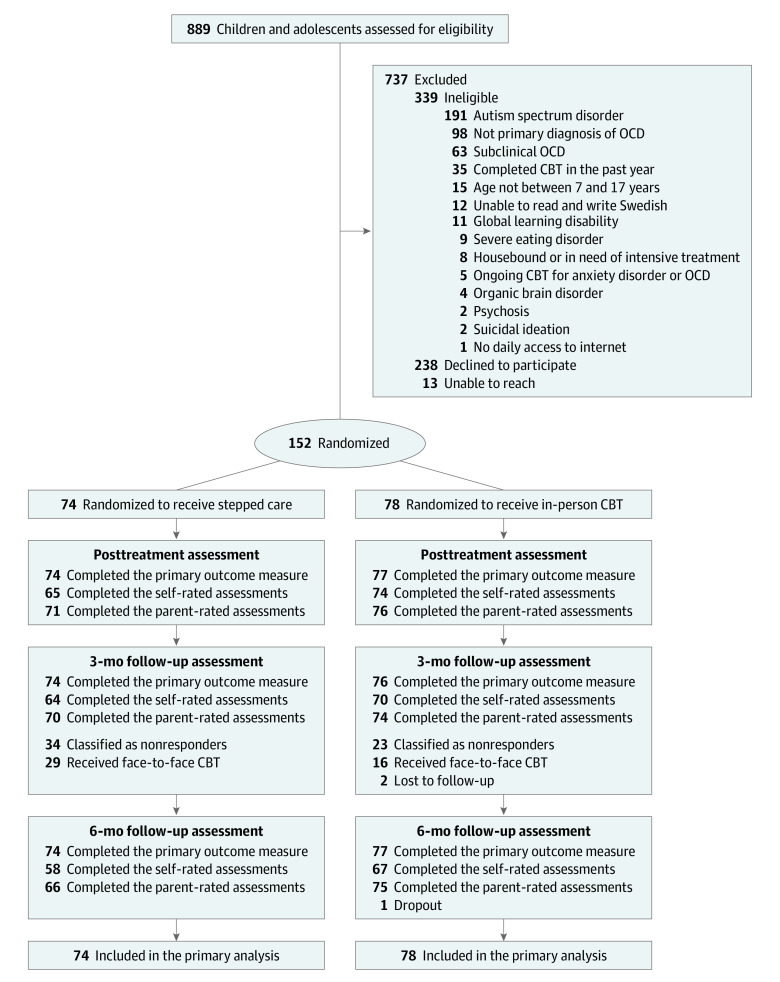
Design, setting and participants: A randomized clinical noninferiority trial conducted at 2 specialist child and adolescent mental health clinics in Sweden. Participants included 152 individuals aged 8 to 17 years with obsessive-compulsive disorder. Enrollment began in October 2017 and ended in May 2019. Follow-up ended in April 2020.
Interventions: Participants randomized to the stepped-care group (n = 74) received internet-delivered CBT for 16 weeks. Nonresponders at the 3-month follow-up were then offered a course of traditional face-to-face treatment. Participants randomized to the control group (n = 78) immediately received in-person CBT for 16 weeks. Nonresponders at the 3-month follow-up received additional face-to-face treatment.
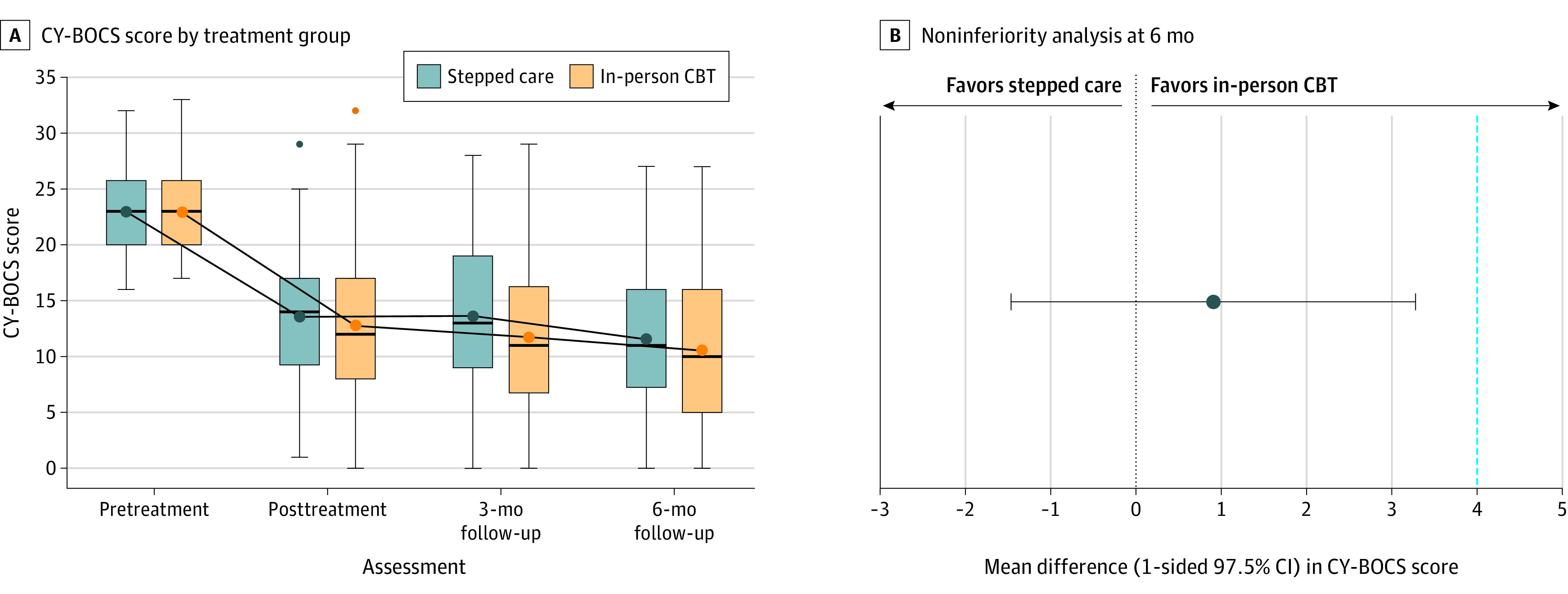
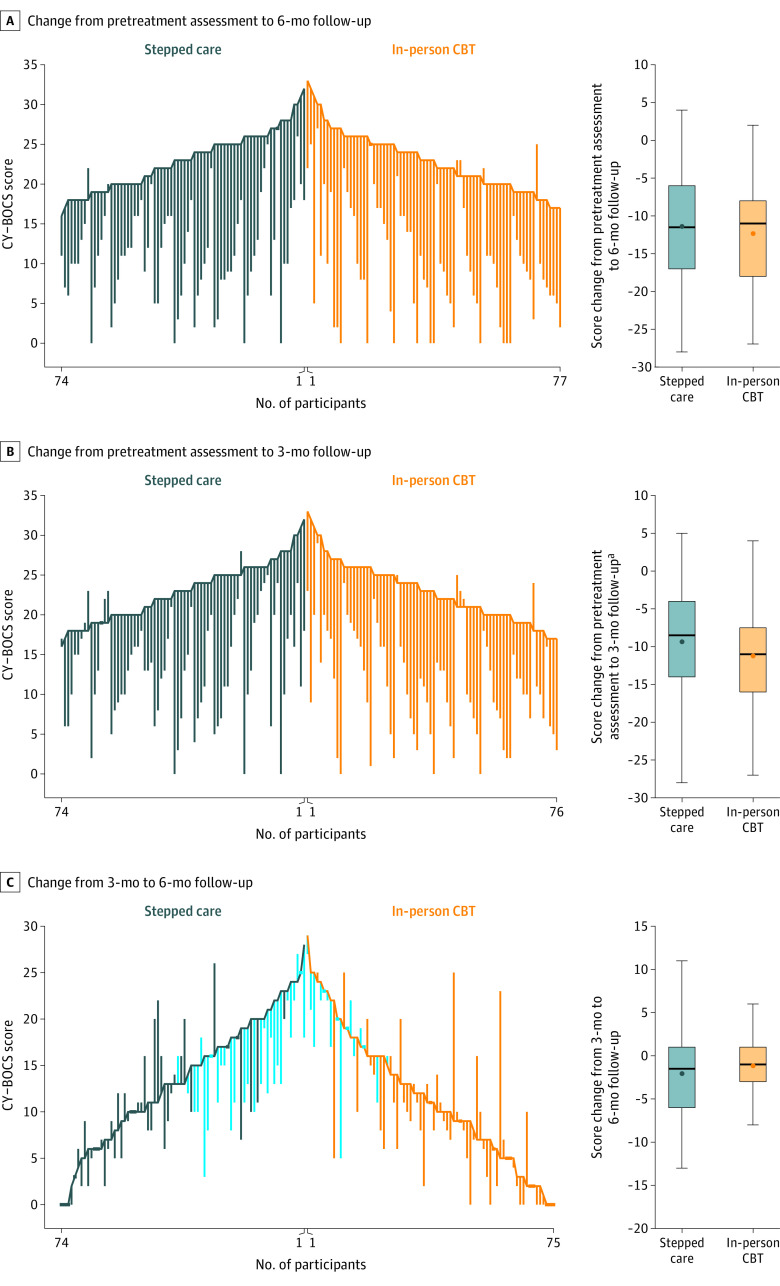
Main outcomes and measures: The primary outcome was the masked assessor-rated Children's Yale-Brown Obsessive-Compulsive Scale (CY-BOCS) score at the 6-month follow-up. The scale includes 10 items rated from 0 (no symptoms) to 4 (extreme symptoms), yielding a total score range of 0 to 40, with higher scores indicating greater severity. Assessors were masked to treatment allocation at pretreatment, posttreatment, 3-month follow-up, and 6-month follow-up assessments. The predefined noninferiority margin was 4 points on the CY-BOCS.
Results: Among the 152 randomized participants (mean age, 13.4 years; 94 [62%] females), 151 (99%) completed the trial. At the 3-month follow-up, 34 participants (46%) in the stepped-care group and 23 (30%) in the in-person CBT group were nonresponders. At the 6-month follow-up, the CY-BOCS score was 11.57 points in the stepped-care group vs 10.57 points in the face-to-face treatment group, corresponding to an estimated mean difference of 0.91 points ([1-sided 97.5% CI, -∞ to 3.28]; P for noninferiority = .02). Increased anxiety (30%-36%) and depressive symptoms (20%-28%) were the most frequently reported adverse events in both groups. There were 2 unrelated serious adverse events (1 in each group).
Conclusions and relevance: Among children and adolescents with obsessive-compulsive disorder, treatment with an internet-delivered CBT program followed by in-person CBT if necessary compared with in-person CBT alone resulted in a noninferior difference in symptoms at the 6-month follow-up. Further research is needed to understand the durability and generalizability of these findings.
Trial registration: ClinicalTrials.gov Identifier: NCT03263546.
Conflict of interest statement
Figures
Comment in
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
